
Victor J. Dzau
The following speech was delivered by Victor J. Dzau, MD, President of the National Academy of Medicine (NAM), at the NAM Annual Meeting in October 2018.
It is my pleasure and honor to be delivering my fourth annual address today as president of the National Academy of Medicine. First I’d like to congratulate three NAM members who have received the 2018 Nobel Prizes in Medicine, Chemistry and Peace: James Allison for his work on cancer immunotherapy, Frances Arnold for her work with the directed evolution of enzymes, and Denis Mukwege for his efforts to end the use of sexual violence as a weapon of war. We are incredibly proud of them as they have all made lasting and life-changing impacts on the world. Now, I’d like to begin with a quote:
“The tragedy of life is often not in our failure, but rather in our complacency; not in our doing too much, but rather in our doing too little; not in our living above our ability, but rather in our living below our capacities.”
These words from Benjamin Mays, often called the father of the modern Civil Rights Movement and a mentor to Martin Luther King, Jr., should be a rallying cry to all of us who have devoted our careers to health and medicine. Like Denis Mukwege, who fought tirelessly against sexual violence in the Democratic Republic of the Congo, we can’t afford to be complacent in 2018, to do too little, or to fail to fully take advantage of the best that science and evidence have to offer. The stakes are simply too high. We are dealing with public health crises on multiple fronts. Overall life expectancy in the U.S. has fallen for two consecutive years — the first decline since the 1960s. Many experts attribute this fall in part to a sharp increase in “deaths of despair,” or lives lost to suicide, alcohol, or drug abuse. Last year, drug overdoses alone killed about 72,000 Americans. Many of these were opioid-related. Consider, too, that we continue to see disturbing health disparities among Americans based on factors such as where they live, socioeconomic characteristics, or racial or ethnic identities. For example, in the U.S. — which has the highest rate of deaths related to pregnancy and childbirth in the developed world — black women are almost four times as likely to die from pregnancy-related causes as white women. As we grapple with these public health crises, we also face challenges on other fronts. There is still much uncertainty about the Affordable Care Act. Public trust in science is fading, evidence is being ignored, and just when we most need them, many researchers and clinicians are not reaching their full potential. They are burnt out or leaving their fields altogether because of overwork, exclusionary policies, and harassment. So, as Dr. Mays so eloquently stated, now is not the time for complacency. Now is the time for action — action based on science and evidence. The National Academy of Medicine is working hard on every one of these issues.
The U.S. Opioid Epidemic
Our work on the opioid epidemic is a powerful example. Since 1999, opioid-related deaths have more than quadrupled. This crisis has taken too many lives, shattered too many families, and ravaged too many communities around the U.S. Although currently there are many efforts occurring at multiple levels, one major barrier to combating the crisis is the fragmentation of efforts and a lack of coordination and collective action. Given the complexity of the issues, solutions have to be multi-sectoral and collective; no single agency or entity can do it alone. In July, the NAM initiated a truly unique Action Collaborative on Countering the U.S. Opioid Epidemic, partnering with the Aspen Institute, to combat the opioid epidemic and galvanize action. We brought together major stakeholders across sectors to collectively develop coordinated, focused efforts to tackle the epidemic — based on evidence of what works. More than 35 organizations including multiple agencies within the U.S. Department of Health and Human Services (HHS), state and local health officials, health care providers, educators and accreditors, pharmacy, and academia have come together to form a public-private partnership. Our collaborative is co-chaired by Admiral Brett Giroir, assistant secretary for health and senior advisor for mental health and opioid policy in HHS; as well as Ruth Katz of Aspen Institute and Jonathan Perlin of HCA Healthcare. The Collaborative is working collectively in four key areas. The first is that we are establishing a coordinated education continuum. To date, education and training have been highly fragmented and variable. This effort will involve educators and accrediting institutions, and be coordinated among undergraduate, graduate and continuing medical education as well as across health professions, including nursing, pharmacy and dentistry. Secondly, we are assisting the U.S. Food and Drug Administration in defining opioid prescribing guidelines for a range of indications and ensuring that these guidelines are successfully translated into workflow. Achieving this requires the collaborative efforts of medical specialty societies: clinicians, pharmacy, and regulators alike. Third, we are addressing how to develop more effective treatment and prevention strategies. These require collaboration among policymakers, care providers, law enforcement, and social services at all levels to achieve progress, as well as a need to build community-based capacity and care models. Finally, we are studying how to support effective research and useful data. There is a need to understand what works and what doesn’t, and to address issues and promote solutions related to data access, sharing, transparency, and interoperability.
Clinician Well Being
Using this same Collaborative model approach, we are taking on another issue that affects the entire health and medical profession: clinician burnout. The statistics are startling: more than 50 percent of physicians are experiencing symptoms of burnout. As many as 30 percent of primary care nurses experience emotional exhaustion, and 24 percent of ICU nurses have post-traumatic stress disorder. That’s not just a terrible burden for these individuals — it’s bad for the quality of patient care. In the past few years, the medical community has started to recognize this problem, and many hospitals, medical centers, and training programs have sprung into action. But these actions have been developed in isolation, and there is little which interventions are effective in addressing this crisis and which are not. In response, we launched the Action Collaborative on Clinician Well-Being & Resilience, a network of more than 60 organizations committed to developing system-level solutions. Our collaborative unites organizations that are already developing individual solutions while bringing new key stakeholders to the table, including policy makers, payers, and vendors of electronic health records. We’re already making a lot of progress. We developed five working groups who have been hard at work addressing the multitude of factors that contribute to clinician burnout, including the regulatory environment, reimbursement, digital health, organizational leadership, and the learning environment. We are working hard to elevate this issue to national attention. In addition, we launched a consensus study to recommend systemic changes to counteract clinician burnout across the entire healthcare system. Nearly 20 years ago, what was then the Institute of Medicine launched two landmark studies — To Err is Human and Crossing the Quality Chasm — which have driven transformative change in health care delivery. We hope that our report on clinician well-being will have a similar impact for the field.
Culture of Health
Another area that is so important for us to address is health equity. Through our multiyear Culture of Health Program sponsored by the Robert Wood Johnson Foundation, we’re working to identify strategies to create and sustain conditions that support equitable good health for everyone in America. In the first three years of the program, we released the report Communities in Action: Pathways to Health Equity, and three more studies are currently under way. We have held many public workshops and community events, and have created tools for stakeholders. As NAM member and former head of the RWJF Risa Lavizzo-Mourey and I wrote in an op-ed, “Americans tend to think of health as an individual responsibility. That’s true, to a point. But that’s not where the responsibility ends. The responsibility for promoting health, and equitable opportunities to achieve it, lies with all of us.” Indeed, we all have a responsibility to fight for better health and health care, especially now.
Vital Directions for Health & Health Care
There is still a lot of uncertainty around the future of the Affordable Care Act, given the many changes enacted by the current administration and in many states. But we can’t afford to lose sight of the values and priorities which our healthcare must provide. These are laid out in the NAM’s Vital Directions for Health and Health Care Initiative which involved 150 experts authoring 20 policy papers on important directions for healthcare. The priorities are: 1) pay for value, 2) empower people, 3) activate communities and 4) connect care. Through this initiative, we are refocusing policy conversations in the nation and especially with policy makers around the issues that matter most for health.
Leadership Consortium for a Value and Science-Driven Health System
Many of the goals of the Vital Directions initiative are carried forward through the NAM’s Leadership Consortium for a Value and Science-Driven Health System. The Leadership Consortium acts as a trusted forum for national leaders in health and health care to work cooperatively.
An Era of Discovery and Innovation
So far, I’ve focused a lot on difficult challenges. But let’s not forget the good news. We are working in an amazing era of scientific discovery, and the potential for revolutionary breakthroughs is extraordinary. We are witnessing rapid scientific and technological progress in areas of genome editing, regenerative medicine, immunotherapy, synthetic biology, 3D printing and more. All hold great promise for future innovative therapies. Furthermore, advances in digital technology, big data and artificial intelligence may improve health care by helping clinicians to make better diagnoses and treatment decisions and by transforming the way patients make personal and health care decisions.
The Grand Challenge for Healthy Longevity
Indeed, as a premier academy of medicine, we consider that an important part of our mission is to stimulate science and innovation to address unmet medical needs especially with the rise of chronic disease and rapid population aging. The NAM Grand Challenge for Healthy Longevity intends to do just that. By 2050, more than 1.6 billion people will be age 65 or older — double the size of the population today — with significant increases in Alzheimer’s and other age-related diseases. We urgently need solutions from research that will keep us healthy, productive, functional, and free of disease as we age. Without action, this could put significant strain on economies, health care systems, and societies around the world. Our Healthy Longevity Challenge aims to address this important issue through an International Commission that will deliver a comprehensive assessment — or “Roadmap” — of the challenges and opportunities presented by global aging, as well as the promising solutions and necessary directions for improving, health, productivity, and quality of life. The Grand Challenge will also stimulate research through a series of inducement prizes and awards to spur innovation. We plan to create Catalyst Awards to incentivize a large base of innovators using the Gates Foundation ‘s Global Grand Challenges as a model. With these $50,000 awards, we plan to support several hundred bold and potentially transformative ideas. They can originate from any field — biology, engineering, social sciences, or a combination of fields. Researchers and innovators can ultimately compete for the Grand Challenge Incentive Prizes of $2 to $5 million each, which will reward breakthrough achievements that dramatically improve human healthspan. We plan to launch the Grand Challenge in early to mid-2019 as a global initiative with the committed participation of up to 30 countries and regions, including Japan, Singapore, the United Kingdom, Taiwan, Hong Kong, and the European Union who are supporting regional competitions for catalyst awards under the umbrella of the NAM Grand Challenge. So we’re off a phenomenal start.
Equitable Scientific Breakthroughs
Just as we need a robust biomedical research enterprise that will produce new medicines and technologies, we also have to ensure that these breakthroughs benefit all of society, and do not exacerbate the inequities we see today. As I wrote in a recent FOCUS paper in Science Translational Medicine, for every new innovation or technology in health, we need to address the larger issues of affordability, access, and equity, as well as potential impact on society. For example, genome editing offers great promise for treating disease, but it also raises complex societal and ethical questions. In 2016, the NAM and the National Academy of Sciences (NAS), along with the Royal Society and Chinese Academy of Sciences, convened an International Summit on this topic. In 2017, we issued a timely report that examined these issues with specific recommendations. Next month, we will hold our Second International Summit in Hong Kong, co-hosted with the NAS, the Academy of Sciences of Hong Kong, and the Royal Society. Indeed, we need to maximize the benefits of scientific and medical breakthroughs and mitigate the risks. To do so, we need to develop policies, norms, standards and incentives that shape the development and deployment of new technologies. As a premier academy in health, science, and medicine, we have an obligation to lead and address these important issues. Our commitment is clearly stated in goal 3 of the 2018-2023 NAM Strategic Plan. Accordingly, we are forming a Committee on Emerging Science, Technology, and Innovation at the NAM, which will examine cutting-edge innovations and technologies in health and medicine through the lens of their potential societal implications.
Speaking Up for Science and Evidence
We also have a duty to speak up when we see that science is being ignored or mi
sused. We are committed to making our voice heard — especially when people’s lives are at risk. Our voice — a voice of reason, objectivity, and of evidence-based solutions — is needed now more than ever. When it became clear, for example, that migrant children were being separated from their families at the U.S.-Mexico border as part of a new immigration policy, we knew the Academy had to speak up. Together with NAS President Marcia McNutt and NAE President Dan Mote, we issued a statement calling for an immediate halt to this practice, citing decades of evidence from National Academies reports that indicates just how serious and lasting the damage could be for these children. In fact, I tweeted on this issue based on my own personal experience. We can’t stay silent on issues such as these, when we know science and research have answers that will help. Gun violence is another example. At least 15,000 people died because of guns last year in the US — and that number excludes suicide. Gun violence is a public health problem that we can do something about. But before we can build solutions, we need to carry out a comprehensive public health research agenda on prevention. In fact, such an agenda was outlined in a 2013 IOM report chaired by NAM member Alan Leshner. Unfortunately, the fraught politics of the issue have prohibited efforts by the U.S. Centers for Disease Control to conduct or support this research. In response to the devastating mass shootings last year, Alan Leshner, Mark Rosenberg, and I co-wrote three editorials reminding policy makers about the IOM report and arguing for federal funding for a comprehensive research agenda on gun violence, which appeared in the Washington Post, Science magazine, and the Annals of Internal Medicine. I am pleased to say that there has been a small but important victory on this front: In the 2018 omnibus funding bill, Congress included explicit language to make it clear that federal support of research on gun violence is allowable, clearing up a long-standing misunderstanding of the Dickey Amendment that resulted in the prohibition of research funding for gun violence for years. But, unfortunately, Congress has yet to allocate the necessary funding to the CDC. We will keep working on this. As an academy, it is also our duty to be a leader and speak out on pressing issues within science and medicine, especially those that threaten our integrity. More than two years ago the National Academies’ Committee on Women in Science, Engineering, and Medicine initiated a study on sexual harassment in academic science, engineering, and medicine. This timely report released 3 months ago, charges academic, research, and professional institutions — including the Academies — to take responsibility by creating a climate of inclusion, diversity, and respect. We have a very important role to play by raising awareness and galvanizing others to follow our lead. We need to disseminate the report’s findings and engage leaders to drive change. I was privileged to participate alongside Paula Johnson, NAM member and co-chair of the sexual harassment study, in a forum at the Aspen Ideas Festival, and we also co-authored an editorial in the New England Journal of Medicine to highlight this issue in the health and medical community. We aren’t stopping there. On November 9, the National Academies will convene a national convocation of academic leaders to discuss what we can do together to end sexual harassment at our own institutions. Going forward, the NAM will work with all of you to continue to speak up for science and evidence-based policy. It’s the right thing to do.
Strategic Plan
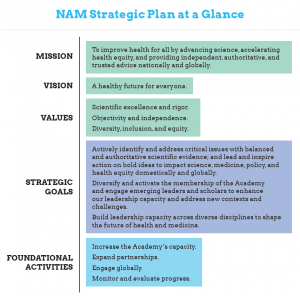
I’m really proud of all that we’ve accomplished together in the past few years. But this is not the time to rest on our laurels. We need to be both vigilant and visionary. We must maintain an unwavering commitment to our core values, but also position ourselves as proactive leaders in a rapidly changing world. Therefore, we recently launched a new strategic plan to position our organization for maximum impact in the coming years. Simply put, our vision is a healthier future for everyone. And we developed a new mission statement:
“To improve health for all by advancing science, accelerating health equity, and providing independent, authoritative, and trusted advice nationally and globally.”
From here on, in everything we do, we will adhere to our core values. We have identified four foundational activities that will be essential for achieving our goals. I’d like to discuss briefly the three strategic goals we have set for ourselves to increase our impact and bring about transformational changes in health and medicine. Our first goal is to actively identify and address critical issues; and lead and inspire action on bold ideas to impact science and medicine, domestically and globally. I’ve already discussed many examples of how we’re meeting this goal: our work on opioids, clinician well-being, culture of health, and healthy longevity to name a few. To be even more proactive in the future, we have created a new NAM committee tasked with identifying emerging opportunities in the basic and translational sciences, and illuminating new
or underrecognized critical issues. Our second goal is to diversify and activate the membership of the Academy and engage emerging leaders and scholars to enhance our leadership capacity. Recently, we have increased the total number of new members who can be elected in any given year, and appointed a diversity committee to help us. We are already seeing progress! Today, we are formally announcing the newest class of 2018 NAM members. This is our most diverse class yet — 42 percent are women, 28 percent are from a minority group, and 24 percent are age 50 and under. Although we are making progress, we recognize that we have much more work to do and we are committed to doing it. We are also considering how to modernize our election process. Frankly, it’s time; we’ve done elections essentially the same way for at least 40 years. Our current membership sections are based on traditional departmental structures and do not necessarily reflect new and emerging areas of science and medicine today, and we need to design a process that recognizes these changes.
We have also started to reach out to the younger generation through our Emerging Leaders in Health and Medicine Program, which we launched in the fall of 2016. We have now named more than 20 exceptional, early- to mid-career professional women and men working in biomedical science, health care delivery, health policy, and related fields, who will lend their energy and expertise to a variety of issues across the National Academies. In April 2019, we will host the inaugural Emerging Leaders Forum, a 2-day event to engage even a wider range of individuals. Members really are the lifeblood of the Academy. Being elected to the NAM is quite an honor, but this honor comes with great responsibility. As individuals, all of us must adhere to the highest ethical standard and conduct ourselves with utmost professional integrity. Sexual harassment or intimidation of subordinates or peers is never acceptable. Fabrication of data or plagiarism is never acceptable. The NAM is taking these issues very seriously. Along with the NAS and NAE, we are developing codes of conduct for our members, including establishing formal mechanisms by which we will address misconduct. Simply put, this is the right thing to do. Our third goal is to build leadership capacity across diverse disciplines to shape the future of health and medicine. As I mentioned earlier, we need to be prepared to embrace new science and align our work with the shape and pace of science today. That’s why we are establishing a new cross-Academies committee on convergence science. A 2016 report from the Massachusetts Institute of Technology described convergence science as “the Future of Health.” Convergence science is described as “an approach to problem solving that integrates expertise from life sciences with physical, mathematical, and co
mputational sciences as well as engineering, merging areas of knowledge from multiple fields to address specific challenges.” Indeed, NAM embraces convergence science to transform health and medicine. However, I believe the current definition of convergence science, focusing on the biology, physical, mathematical and engineering sciences, is too narrow. As I pointed out in a recent paper in the Lancet, we have to expand this definition of convergence for all areas of health. For example, we need to reimagine population health in terms of convergence. We need to draw on social, behavioral, economic, data, legal, and political sciences, to name a few to converge on research, policy, and implementation — all with the goal of influencing population health outcomes.
Looking to the Future
So I hope you’ll agree that in the three short years since we have become an academy, we have been far from complacent. We have established our own identity as the nation’s premier advisor on matters related to health and medicine. And we are tackling the really tough issues that matter in society, now and in the future. As the IOM and now as the NAM, we will be celebrating the 50th anniversary of our founding in 2020. This provides the perfect opportunity to not only celebrate all that we’ve accomplished together, but also begin to chart a course for the next 50 years of U.S. and global leadership in health and medicine. In order to continue in our impressive trajectory and impact as a world-class academy, we will need robust resources and support. We are grateful that the federal government continues to seek us out for objective advice, but we can’t rely solely on government to support some of the really important work that needs to be done. We want to continue to be proactive in identifying and tackling issues that will really have an impact and lay the foundation for better health for everyone. And we need resources to do that. That is why we have started a major development campaign to raise $100 million over 7 years. We are just beginning the silent phase and plan to launch the public phase in 2020 to coincide with the 50th Anniversary. Our goal of $100 million is an ambitious goal, to be sure, but it’s entirely within the realm of the possible. And it’s really necessary if we want to continue doing the excellent work we do. You will be hearing much more about this campaign in the coming months. I’ve covered a lot of ground today, but let me conclude by saying a heartfelt “thank you.” I am so grateful to our members, to our sponsoring organizations, and to our volunteers and members of the public who support us. It is because of your commitment, your dedication, and your hard work that we have accomplished all that we have. There’s an old Chinese proverb: “A single tree does not make a forest. A single string cannot make music.” We can accomplish a lot as individuals, but when we come together through the National Academy of Medicine and work toward common goals, we make the seemingly impossible, possible. Through our work, we are shaping not only our own destiny, but that of future generations here and around the world. I look forward to serving all of you for the next several years to ensure the realization of our plans and reach our full potential as the world’s leading academy of medicine.
