Assessing Meaningful Community Engagement
Research Engagement Survey Tool
KEY FEATURES
COMMUNITY/ GEOGRAPHY
Stakeholders in community-engaged research
United States
COMMUNITY ENGAGEMENT OUTCOMES
Strengthened partnerships + alliances
Diversity + inclusivity
Acknowledgment, visibility, recognition
Sustained relationships
Mutual value
Trust
Shared power
Structural supports for community engagement
Expanded knowledge
New curricula, strategies + tools
Bi-directional learning
Community-ready information
Improved health + health care programs + policies
Community-aligned solutions
Sustainable solutions
PLACE(S) OF INSTRUMENT USE
Community/community-based organization (intended)
LANGUAGE TRANSLATIONS
Not specified
PSYCHOMETRIC PROPERTIES
Content validity
YEAR OF USE
2017-2019
Assessment Instrument Overview
The Research Engagement Survey Tool (REST) has 32 questions and is used by community health stakeholders. It evaluates the quality and quantity of stakeholder engagement in research. REST was modified from another instrument: the Community Engagement Measure.
Alignment with Assessing Meaningful Community Engagement Conceptual Model
The questions in REST were realigned to the Assessing Community Engagement Conceptual Model. Figure 1 displays the alignment of REST with the Conceptual Model domain(s) and indicator(s). Where an instrument is mapped broadly with a domain or with a specific indicator, the figure shows the alignment in blue font.
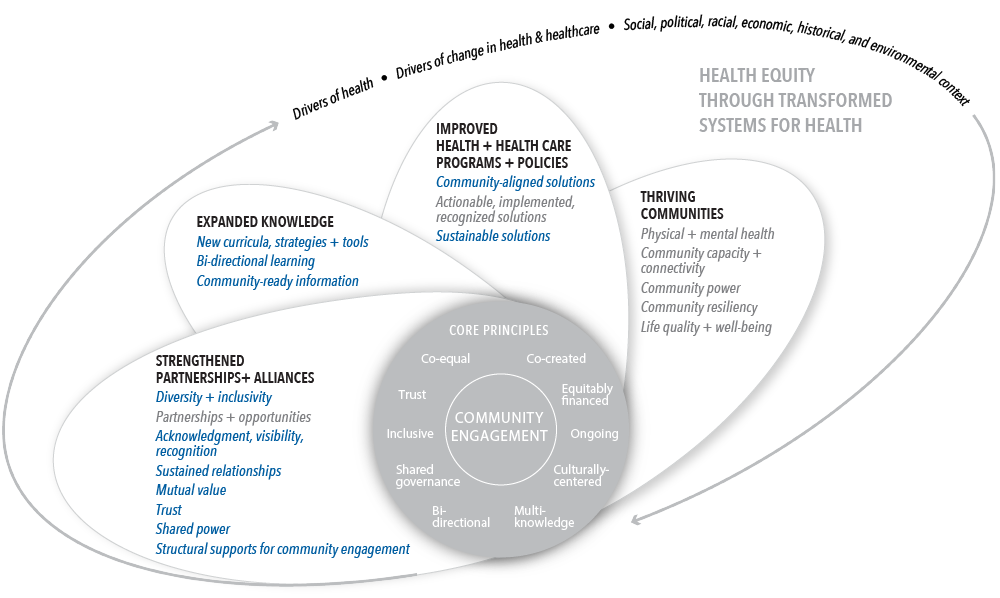
Table 1 displays the alignment of REST’s individual questions with the Conceptual Model domain(s) and indicator(s). The table shows, from left to right, the aligned Conceptual Model domain(s) and indicator(s) and the individual questions from REST transcribed as they appear in the instrument (with minor formatting changes for clarity).
| CONCEPTUAL MODEL DOMAIN(S) AND INDICATOR(S) | ASSESSMENT INSTRUMENT QUESTIONS |
| STRENGTHENED PARTNERSHIPS + ALLIANCES; Diversity + inclusivity | 1.1: Focus on issues important to the community. 1.3: Incorporate factors (for example—housing, transportation, food access, education, employment) that influence health status, as appropriate. 1.4: Focus on cultural factors that influence health behaviors. 5.1: Build on strengths and resources within the community or patient population. 5.2: Work with existing community coalitions and organizations. 5.3: Team includes representation from the local community or patient population. |
| STRENGTHENED PARTNERSHIPS + ALLIANCES; Acknowledgment, visibility, recognition | 6.4: Treat all partners’ ideas with openness and respect. 8.2: Partners are confident that they will receive credit for their contributions to the partnership. |
STRENGTHENED PARTNERSHIPS + ALLIANCES; Sustained relationships | 3.3: All partners share updates, progress, strategies, and new ideas regularly. |
| STRENGTHENED PARTNERSHIPS + ALLIANCES; Mutual value | 4.3: The partnership adds value to the work of all partners. 8.3: Mutual respect exists among all partners. 8.4: All partners respect the population being served. 8.5: Partners understand the culture of the organizations and community(ies) involved in the partnership. |
| STRENGTHENED PARTNERSHIPS + ALLIANCES; Trust | 8.1: The environment fosters trust among partners. |
| STRENGTHENED PARTNERSHIPS + ALLIANCES; Shared power | 1.2: Examine data together to determine the health problems that most people in the community think are important. 2.1: all partners assist in establishing roles and responsibilities for the collaboration. 2.2: All partners have the opportunity to share ideas, input, leadership responsibilities, and governance (for example—memorandum of understanding, bylaws, organizational structure) as appropriate for the project. 2.4: Through mutual agreement, partners take on specific tasks according to their comfort, capacity, and expertise. 3.4: Plan for ongoing problem solving. 3.5: Involve all partners in determining next steps. 4.4: Partners share resources to build capacity. 6.1: Establish fair and equitable processes to manage conflict or disagreements. 6.2: All partners are comfortable with the agreed‐upon timeline to make collaborative decisions about the project. 6.3: Partners agree on ownership and management responsibility of data and intellectual property. 7.1: All partners have the opportunity to be coauthors when the work is published.* 7.3: Involve interested partners in dissemination activities.* |
| STRENGTHENED PARTNERSHIPS + ALLIANCES; Structural supports for community engagement | 7.1: All partners have the opportunity to be coauthors when the work is published.* 7.3: Involve interested partners in dissemination activities.* |
| EXPANDED KNOWLEDGE; New curricula, strategies + tools | 4.1: All partners have a variety of opportunities to gain new skills or knowledge from their involvement. |
| EXPANDED KNOWLEDGE; Bi-directional learning | 4.2: Encourage all partners to learn from each other. |
| EXPANDED KNOWLEDGE; Community-ready information | 7.2: The partners can use knowledge generated from the partnership. |
| IMPROVED HEALTH + HEALTH CARE PROGRAMS + POLICIES; Community-aligned solutions | 2.3: Plans are developed and adjusted to meet the needs and concerns of the community or patient population. 3.1: Continue community‐engaged activities until mutually agreed‐upon goals are achieved. |
| IMPROVED HEALTH + HEALTH CARE PROGRAMS + POLICIES; Sustainable solutions | 3.2: Partners continue community‐engaged activities beyond an initial project, activity, or study. |
*Note that these questions are duplicated to reflect their alignment with multiple domains and/or indicators in the Conceptual Model.
Table 1 | Research Engagement Survey Tool questions and alignment with the domain(s) and indicator(s) of the Assessing Community Engagement Conceptual Model
ASSESSMENT INSTRUMENT BACKGROUND
Context of instrument development/use
Using a stakeholder‐engaged approach, this study validated content to ensure that the tool is testing what it is intended to evaluate, as well as item reduction to determine which items should be removed or reduced from the quantitative measure of research engagement. “A broad range of stakeholders (e.g., patients, caregivers, advocacy groups, clinicians, researchers) who have experience with and knowledge about community‐engaged research” participated in an iterative approach to identify what matters most to them. The stakeholders also included one community member who was new to community-engaged research and could provide the perspective of someone who did not have prior research experience.
Instrument description/purpose
REST is intended for community health stakeholders participating in research and assesses the quality and quantity of stakeholder engagement in research using nine areas of focus:
- Partner input is vital
- Partnership sustainability to meet goals and objectives
- Build on strengths and resources within the community or patient population
- Foster co‐learning, capacity building, and co‐benefit for all partners
- Facilitate collaborative
- Equitable partnerships
- Involve all partners in the dissemination process
- Build and maintain trust in the partnership
- Focus on community perspectives and determinants of health.
REST has 32 questions to measure “how well the partners leading the research” conduct certain activities and “how often the partners leading the research” conduct certain activities. The five-point Likert scales range from “poor” to “excellent” and “never” to “always,” respectively.
REST can be accessed here: https://wp.nyu.edu/collegeofglobalpublichealth-goodman_mle_lab/rest/.
Engagement involved in developing, implementing, or evaluating the assessment instrument
A 19-person panel composed of a broad range of stakeholders was recruited. The panel comprised patients, caregivers, advocacy groups, clinicians, and researchers with experience with and knowledge about community-engaged research, as well as one community stakeholder with no prior research experience. They were identified by email based on the networks of the project team members and served as a convenience sample for the project. Additionally, while the initial panel included a majority of academics, the final panel included additional community partners who were recommended by the academics. Using an iterative process to capture the interests of panel members that included online surveys, in-person meetings, and webinars, the panel arrived at a consensus on the items corresponding to eight areas to be used in REST to measure community engagement in research. Each item in the tool had greater than 80% agreement among group members during the process.
Additional information on populations engaged in instrument use
After the first round of the iterative process, one panelist was not able to continue to participate. “The remaining 18 panelists remained engaged in the process. …The resulting panel sample was majority female (90%), non‐Hispanic (95%), African‐American or Black (63%), with some college or higher education (100%) and resided in the Midwest or Southern region of the United States (72%).”
Notes
- Potential limitations: The panel was recruited using a convenience snowball sampling approach based on the networks of the project team members. The panel’s views do not represent all ethnic groups or gender identities (e.g., Asian, Native American, and transgender), which may influence the content validation process. Further, other identities (e.g., health professions and disciplines not included; limited English proficiency; nationality; sexual orientation; health status) were not involved in the development of REST and “the impact of their presence or absence is unknown.”
- Important findings: REST has undergone comprehensive validation and identifies “common standardized evaluation metrics.” It can be used across and within projects and over time to track progress on engagement and to ensure that all aspects across the project’s translational continuum are grounded in engagement.
- Supplemental information: Additional information on REST and additional populations in which the instrument was tested can be found in the following articles and reports:
- NYU School of Public Health. n.d. REST: Research Engagement Survey Tool (REST). Available at: https://wp.nyu.edu/collegeofglobalpublichealth-goodman_mle_lab/rest/ (accessed July 14, 2022).
- Goodman, M. S., N. Ackermann, K. A. Pierce, D. J. Bowen, and V. S. Thompson. 2021. Development and Validation of a Brief Version of the Research Engagement Survey Tool. International Journal of Environmental Research and Public Health 18(19). https://doi.org/10.3390/ijerph181910020.
We want to hear from you!
Assessing community engagement involves the participation of many stakeholders. Click here to share feedback on these resources, or email [email protected] and include “measure engagement” in the subject line to learn more about the NAM’s Assessing Community Engagement project.
Related Products
