

Introduction
In 2015, the Institute of Medicine (now the National Academy of Medicine) released the report Vital Signs: Core Metrics for Health and Health Care Progress as a “basic, minimum slate of core metrics for use as sentinel indices of performance at various levels with respect to the key elements of health and health care progress” (IOM, 2015). Although indicators of pediatric health were included in that report as key elements of healthy behaviors, healthy communities, and preventive services, the core measures in the report emphasized indicators of adult health. This series of papers, “Vital Signs for Pediatric Health”, describes four metrics across the pediatric life course, each measuring how well the health care system is building the physical, cognitive, and socio-emotional health of the pediatric population, thereby laying the foundation for life-long health and well-being. The metrics—infant mortality, school readiness, chronic absenteeism, and high school graduation—were selected to focus on four different developmental stages of growth. A standardized set of core metrics to assess pediatric health could provide data to support health systems in identifying important areas for attention among their pediatric population and enable them to respond in a timely way. This rapid response is especially important in pediatric health systems as children undergo rapid development within a short time span.
This paper discusses one of those four measures—chronic absenteeism in middle school—as a developmental target for middle childhood. Middle school may include grades 5 to 9 or a subset of these grades; typically, this includes children who are approximately 10–15 years old. While chronic absenteeism—typically defined as missing 10% or more of enrolled school days—has potential utility as a measure from the time children enter formal schooling in pre-kindergarten through grade 12, measuring chronic absenteeism in middle childhood provides critical information about health and well-being between two key developmental stages captured by other vital signs: early childhood, captured by school readiness, and adolescence, captured by high school graduation.
Health and educational success are intertwined, as more education has been linked to better health outcomes across the life course (Basch, 2011; Cutler and Lleras-Muney, 2006). Therefore, participation in education is crucial for both developmental and educational progress. Research has documented associations of chronic absenteeism with both acute (e.g., influenza infection, fractures) and chronic (e.g., asthma, type 1 diabetes mellitus) physical health conditions, as well as with mental health disorders and substance use (Allison et al., 2019). Research has also linked chronic absenteeism to poorer educational performance and attainment (Allison et al., 2019). Chronic absenteeism is robustly inversely associated with on-time high school graduation (BERC, 2011). For more information on the importance of high school graduation, refer to “Vital Signs for Pediatric Health: High School Graduation” (Hoagwood et al., 2023).
Given the links between educational attainment and health, measuring students’ chronic absenteeism in middle school may provide a window into physical and mental health in middle childhood and early adolescence, socioemotional functioning, readiness to learn, family risk and resilience, and potential threats to current and long-term health and well-being (RWJF, 2016). School-level chronic absenteeism, as well as aggregations of multiple schools, such as those served by a particular health system, may also provide an indicator of the adequacy of interventions to promote health and educational equity at the population level. As such, chronic absenteeism could be a vital sign to measure health systems’ performance.
The remainder of this paper defines the chronic absenteeism measure, the selection of the specific measure that assesses chronic absenteeism, and the technical integrity of the measure. The paper also makes clear the links between school attendance and individual health outcomes. The shifting landscape of chronic absenteeism in the COVID-19 global pandemic and its anticipated aftermath are also considered.
Defining Chronic Absenteeism
In the 2013–2014 school year, the Office of Civil Rights began collecting and aggregating national student absence data using a biennial survey of schools as part of the U.S. Department of Education’s (DOE) Civil Rights Data Collection (CRDC) (DOE CRDC, 2018). The CRDC defined chronic absenteeism as missing 15 or more school days per school year. However, experts noted that different school districts had different numbers of school days and waiting until a student amassed 15 missed school days did not lend itself to ongoing monitoring and early intervention. Thus, experts urged for the definition of chronic absenteeism be adapted to missing 10% or more of enrolled school days (Chang et al., 2018; Lara et al., 2018). This change was adopted with the passage of the 2015 Every Student Succeeds Act (ESSA), the federal education law that replaced No Child Left Behind.
Under ESSA, alongside academic metrics, all states must report chronic absenteeism data. States must also collect one nonacademic indicator of school quality or student success (Jordan and Miller, 2017). ESSA stipulates that this non-academic indicator must be:
- evidence-based;
- valid and reliable across school districts in a given state; and
- related to student learning, achievement, graduation, and
post-secondary matriculation.
Most states use the required measure of chronic absenteeism as their non-academic indicator, as a proxy measurement for student engagement (DOE, 2019; Jordan and Miller, 2017).
Beginning in the 2017–2018 school year, the DOE shifted monitoring of chronic absenteeism from the CRDC to its EdFacts initiative (a DOE effort “to collect, analyze, and promote the use of high-quality, pre-kindergarten through grade 12 data” [DOE, 2023]). Data are aggregated from schools by states using electronic student information systems with standard definitions to increase data quality (Attendance Works and Everyone Graduates Center, 2021). Data are collected during the summer following a given school year and published the following fall or winter, more rapidly than the CRDC data. Therefore, chronic absenteeism is an administratively collected indicator of student and school performance across the U.S., facilitating its use as a pediatric vital sign (Schanzenbach et al., 2016).
The DOE’s current definition of chronic absenteeism being when a student misses 10% or more of enrolled school days allows students at risk for chronic absenteeism to be identified at any point in the school year and allows comparisons of the metric across geography, health systems, and time (Allison et al., 2019; Connolly and Olson, 2012). The ability to assess chronic absenteeism at any point will allow for the capture of data on students who may not remain in school for an entire year (such as students in the child welfare system and those experiencing housing instability or homelessness). Unlike truancy, which captures only unexcused absences, chronic absenteeism captures all days a student is absent from school, regardless of the reason. Both excused and unexcused absences are counted (e.g., illness days, family vacations) when documenting chronic absenteeism, as are disciplinary absences (e.g., out of school suspensions) (Bauer et al., 2018). Chronic absenteeism differs from average daily attendance, which captures how many students in a school attend each day. Average daily attendance is a school-level metric that does not allow for the identification of students whose absenteeism puts them at academic, social, and health risk. For example, even if a school has 95% average daily attendance, 30% of students could still be chronically absent (Bruner et al., 2011).
There is precedent for using school absences as a measure of population health and well-being in early adolescence. Reducing chronic school absence among early adolescents is an indicator in the U.S. Department of Health and Human Services’ Healthy People 2030 goals for the nation’s health (CDC, 2020). The Healthy People 2030 goal defines chronic absenteeism as missing three or more whole days of school in the last month, based on student self-report in an annual assessment. School absenteeism was also included in Healthy People 2020 goals, as assessed by the number of adolescents aged 12 to 17 years who missed 11 or more whole school days during the preceding 12 months because of illness or injury, based on self-report data from the National Health Interview Survey.
Selecting Chronic Absenteeism as a Pediatric Vital Sign
As described above, student absence data are already collected by school districts for monitoring and accountability purposes; the measure is intuitive and non-technical; it is meaningful across development from pre-kindergarten to grade 12; and it can provide a window into student and school functioning and developmental status that encompasses a variety of academic, social, and family domains. Students may miss school due to family obligations, illness, trauma, housing instability, lack of access to reliable transportation, competing work responsibilities, or juvenile justice system involvement (Balfanz and Byrnes, 2012). Reducing chronic absenteeism could focus attention on solutions that engage families, educators, health care providers, and health systems in addressing issues relevant for specific populations of children. Students may also miss school because of lack of safety at school (such as exposure to bullying and harassment), lack of engagement with school, or because they or their parents do not value school attendance or are not aware of how much school they are missing (Rogers and Feller, 2016; Balfanz and Byrnes, 2012). Thus, beyond the risk and resilience of students, chronic absenteeism can also provide insight into the risk and resilience of schools and school districts.
A possible alternative metric to chronic absenteeism is truancy, or the number of unexcused absences. However, truancy has historically included legal and administrative punishments for students and their parents, whereas this is not the case for chronic absenteeism (Attendance Works, 2018). Parents whose children do not attend school may be referred to truancy court, where they can be fined. Those who are unable to pay truancy fines may be sentenced to serve jail time, exacerbating economic and social problems that are often the root causes of absenteeism (Weathers et al., 2021). Prior research suggests that truancy court programs are largely ineffective, and involvement with the justice system is itself associated with a lower likelihood of attending school (Attendance Works, 2020b; Lee et al., 2016). Chronic absenteeism is also highly correlated with trauma, and research shows that an empathetic response rather than a blaming response often leads to increased school attendance (Attendance Works, 2020b). An asset-based school accountability framework focused on facilitating attendance may motivate improved partnership with parents on strategies such as home visits, providing or arranging transportation, health care referrals, or support and referrals for unmet social needs (Attendance Works, 2018; Rogers and Feller, 2016). Thus, using chronic absenteeism as a vital sign, rather than truancy, may be more supportive of family and community well-being.
Recent Data and Trends in Chronic Absenteeism
In 2015–2016, 10% of students nationwide were chronically absent, based on the definition at the time of 15 absent days or more during the school year (Chang et al., 2018). The number of students considered chronically absent increased by approximately 800,000 between 2013–2014 (the first year of CRDC data collection) and 2015–2016 (Chang et al., 2018). Much of this increase was explained by better reporting: the proportion of schools that reported that they had no chronically absent students declined precipitously between 2013–2014 and 2015–2016, increasing confidence in the quality of the data (Chang et al., 2018). Unfortunately, because CRDC data collections in 2013–2014 and 2015–2016 relied on a different definition of chronic absenteeism, 2017–2018 data cannot be compared directly with prior years.
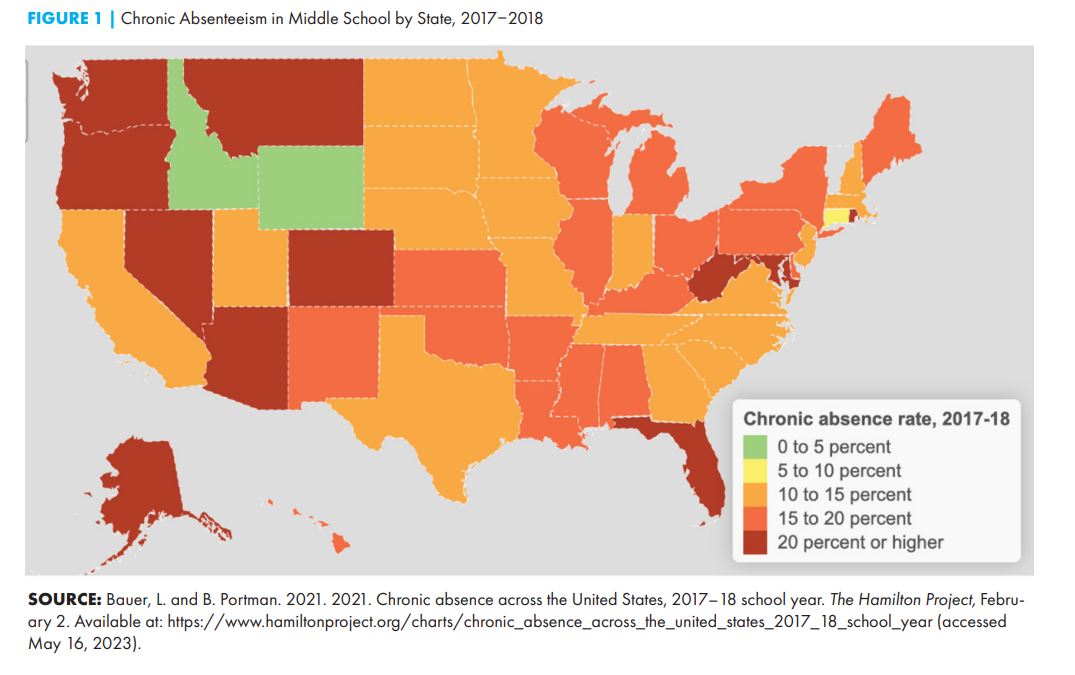
In the 2017–2018 school year, the first year that federal data were reported by EdFacts using the definition of chronic absenteeism based on 10% of enrolled days, 13.9% of middle school students were chronically absent nationwide. However, this value obscured substantial variation by state and school (see Figure 1). About half of the students who were chronically absent attended schools in which 20% or more of students were chronically absent (Attendance Works and Everyone Graduates Center, 2021). The state with the highest rate of chronic absenteeism (Alaska with 28.9%) had a rate more than 15 times higher than the state with the lowest rate (Wyoming with 1.9%) (DOE CRDC, 2019).
School health and safety protocols during the COVID-19 pandemic introduced new questions about data quality and appropriate ways to measure absenteeism going forward. In spring 2020, schools pivoted to remote learning models as a public health precaution. In a national survey of teachers in May 2020, 97% of respondents reported that their schools were closed for in-person instruction (Educators for Excellence, 2020). The COVID-19 pandemic continues to widen deep existing inequalities, with disproportionate impacts on low-income students and students of color (Goudeau et al., 2021; Ambrose, 2020).
During the COVID-19 pandemic, many students and their families faced severe economic stressors, housing and food insecurity, grief, loss of and separation from loved ones, and illness for themselves and their family members (CDC, 2022). For many families where a caregiver was an essential or shift worker, lack of adult supervision proved a major barrier to consistent participation in remote school (Reich et al., 2020). Alongside the reorganization of family life during COVID-19, low-income students and those from historically marginalized racial and ethnic groups were also caught in the “digital divide,” as many lacked an appropriate and accessible device (computer, tablet) for their schoolwork and reliable internet to participate in remote learning (Lai and Widmar, 2020).
Both attendance and the measurement of attendance changed due to the COVID-19 pandemic. In May 2020, 32% of teachers in a national survey reported that no more than half of their students participated daily in distance learning (Educators for Excellence, 2020). Moreover, the survey revealed that it was not just students whose schools offered full-time remote learning who were likely to be absent—absenteeism was also up in schools that were open for in-person instruction. During remote learning, absence policies were in flux. By the end of 2020, about 60% of states reinstated requirements to take daily attendance, and the other 40% required less frequent attendance taking or allowed districts to use their discretion (Attendance Works and Everyone Graduates Center, 2021). Schools continue to grapple with unexcused and unverified absences as well as absences due to COVID-19 quarantine and isolation measures (Attendance Works and Everyone Graduates Center, 2021). Therefore, at least in the short term, data on chronic absenteeism may be fragmented and more complicated to interpret than before the COVID-19 pandemic.
Disparities
Chronic absenteeism is found among students of every race and ethnicity but disproportionately affects specific student populations. Recent national data has shown that American Indian students were 81% more likely to be chronically absent than their White peers, Pacific Islander students 50% more likely, and Black students 44% more likely (Attendance Works and Everyone Graduates Center, 2021). Racial and ethnic disparities vary by state, however, with some states showing White students more likely to be chronically absent compared to Black students (Chang et al., 2018). Emerging state-level data suggest that the COVID-19 pandemic has exacerbated disparities in chronic absenteeism. In Connecticut, for example, a preliminary analysis showed that chronic absenteeism more than doubled among English language learners and increased 75% among students eligible for free and reduced-price meals in the 2020–2021 school year compared to the prior year (Chang et al., 2021).
Before the pandemic, chronic absenteeism was three to four times higher among low-income students, who may most benefit from being in school (Balfanz and Byrnes, 2012; Chang and Romero, 2008). National data suggest a correlation between school poverty levels and chronic absenteeism, with poverty being a stronger determining factor than location. The literature shows that high rates of chronic absenteeism among those living in poverty are likely due to an array of parental and family risks, including single-parent households, low parental education, family unemployment, food insecurity, poor family health, and having multiple siblings (Chang and Romero, 2008). However, there is variability in chronic absenteeism rates among low-income communities, suggesting that there may be child and family factors operating alongside issues related to schools or communities that may serve as either risk or protective factors.
Students who are at risk for lower educational attainment (e.g., those in special education, alternative, and vocational programs) are more likely to be chronically absent. In 2017–2018, students receiving services under the Individuals with Disabilities Education Act had a chronic absence rate of 23.4%, 46% higher than students overall (Attendance Works and Everyone Graduates Center, 2021). Improving attendance rates for students with disabilities requires different and potentially individualized interventions than those for the rest of the population.
Historically, the kindergarten grade level has a high chronic absenteeism rate that decreases over the elementary grades, with the lowest levels in 3rd and 4th grade. The chronic absenteeism rate then increases through middle and high school grades with a peak at 12th grade (Balfanz and Byrnes, 2012). Specific school and developmental transitions are correlated with higher rates of chronic absenteeism, including the start of formal education, transitions into middle and high school, and the senior year of high school before graduation. Data from 2017–2018 illustrate an alarming trend for older students, in that half of the high schools in the U.S. have chronic absenteeism rates of 20% or higher (Attendance Works and Everyone Graduates Center, 2021).
Changes in Measuring Chronic Absenteeism
There are several challenges associated with measuring chronic absenteeism. First, as described above, is the challenge of the changing definition of the measure that precludes comparing data before and after the 2017–2018 school year. The current definition, missing 10% or more of enrolled school days, has advantages including ease of comparison across states with different numbers of school days and increased ability to capture absence among highly mobile student populations. The second challenge is that while low absenteeism indicates that students are on average attending some period of the school day, it does not measure whether they are engaged in classroom activities while present and whether their learning and psychoeducational needs are being met. The third challenge is related to the COVID-19 pandemic. There are now more ways that students can attend school. Some fraction of students and families will continue to pursue remote learning options even after the COVID-19 pandemic subsides, including those who have children who thrived in remote school (Lockee, 2021). Given the high prevalence of structural and logistical barriers to full participation in remote school during the pandemic, counting absences during remote learning proved challenging (Attendance Works and Everyone Graduates Center, 2021). The steps for remote learning engagement outlined in Figure 2 include parent participation, availability of a device, access to quality broadband internet, digital competency to set up and log into classes, attendance, and remote learning engagement and participation. Attendance Works, a national and state initiative to promote school attendance, has proposed four additional metrics to supplement chronic absence for remote learning:
- contact (ability to reach student);
- connectivity (access to digital resources and competency);
- relationships (ability to establish school-family connections and relationships); and
- participation (participation in learning and educational opportunities) (Attendance Works, 2020a).
While these supplemental metrics could allow for greater insight into students’ and families’ engagement with school and broader recognition of barriers to full and equitable participation, they also complicate the measure of chronic absenteeism by introducing new factors that must be considered.
A fourth challenge to using chronic absenteeism as a health system indicator is the limited scale at which the measure is available for use by health systems. The unit of aggregation at which chronic absenteeism is reported may vary from the school level to the school district level. Children in a single health system might attend a variety of schools whose geographical catchment may not overlap with the health care systems’ rolls. Pilot projects exist that worked to include chronic absenteeism in the pediatric primary care electronic health record, which would allow for tailored aggregation (NASEM, 2019). Efforts to link data systems might facilitate better alignment between the geography of chronic absenteeism and the geography of health systems’ catchment areas. Data linkages and sharing would be governed by applicable privacy protections, including the Family Educational Rights and Privacy Act and the Health Insurance Portability and Accountability Act (see [PHII, 2020] for clarification on privacy requirements).

Importance of Measuring Chronic Absenteeism to Understand Children’s Health
Linkages to Outcomes Later in Life
Across the life course, chronic absenteeism in middle childhood is linked to adult health primarily through disrupting educational success and attainment. In turn, less educational success and attainment predict poorer health (Cutler and Lleras-Muney, 2006). Chronic absenteeism among children may also affect parental ability to work and may thereby disrupt parent health and family economic stability.
Consistent attendance helps facilitate progress toward on-time high school graduation. A study of students in New York City found that attendance during middle school predicted students being on track in 9th grade to graduate high school in four years (Kieffer et al., 2011). In Baltimore, only 36% of 6th graders who missed 20 to 39 days of school graduated within one year of on-time graduation (BERC, 2011). In Philadelphia, only 17% of 6th graders who were present for less than 80% of school days graduated within one year of on-time graduation (Balfanz et al., 2007). High levels of chronic absenteeism may undermine achievement across the entire school population, not just the achievement of students who are absent (Musser, 2011).
By the time students enter high school, chronic absenteeism is among the most robust predictors of school dropout—more predictive than suspensions or test scores, even after accounting for other student characteristics (Allensworth and Easton, 2007). Attendance does not just matter for students who are struggling academically. 9th grade students with high standardized test scores who missed two or more weeks of school were more likely to fail than students with low test scores who missed a week or less of school (Allensworth and Easton, 2007).
Students who are chronically absent from school are also more likely to engage in health risk behaviors. Absenteeism has been associated with increased risk of using alcohol, tobacco, marijuana, and other drugs, as well as risky sexual behavior (Eaton et al., 2008; Guttmacher et al., 2002; Hallfors et al., 2002). Absenteeism has also been linked to greater risk of unintentional and intentional injuries (Eaton et al., 2008). There is some evidence that type of absence also matters. In a meta-analysis, unexcused absences were positively associated with substance use, particularly among middle school-aged students (Hallfors et al., 2002). Finally, though there are multiple reasons for chronic absenteeism, poor mental or physical health or other family and social risks are likely to be contributory (Allison et al., 2019; Jacob and Lovett, 2017). Thus, chronic absenteeism may be an important indicator of the need for health and social services.
Potential Health Systems Benefits
In order to address the root causes of chronic absenteeism, a broader systems approach to coordinate and build connections between individual, family, school, and community factors that may contribute to absenteeism is required (Balfanz and Byrnes, 2012; Ingul et al., 2012). While chronic absenteeism is reported as an educational measure, in many cases the causes may be external to the education system itself, including underlying health status, family circumstances, and housing instability (Balfanz and Byrnes, 2012). Many health conditions have been associated with school absenteeism, ranging from acute illness to chronic pain to mental health conditions to poor oral health, and children with special health care needs may have more school absences than children without special health care needs (Forrest et al., 2011). However, limited data exists on which health conditions may be more likely to result in higher rates of absenteeism, and additional research could help clarify which conditions are most related to chronic absenteeism (Jones et al., 2009). In addition, mental health conditions have also been associated with school absenteeism, and inversely, school absenteeism may lead to depressive symptoms (Wood et al., 2012).
Managing chronic absenteeism will likely require a multilevel and multisector approach to support optimal child health and development and to eliminate equity gaps. Monitoring chronic absenteeism may provide insight into unmet health and social needs and the adequacy of health care access and developmental supports from the individual to population level. As such, a deeper understanding of chronic absenteeism may help motivate increased collaboration among population health, primary and specialty care clinicians, and educational stakeholders to meaningfully improve child and family outcomes. Further opportunity exists to consider how all elements of a larger framework, inclusive of individual, family, and school factors, contribute to school attendance. While the medical neighborhood (the partners and contexts that support a patient-centered medical home) has initially focused on groups of physicians under the same management, a pediatric-focused medical neighborhood, which expands this definition to include enhanced collaboration with distributed leadership among medical, home, school, and community-based partners, may be a population health approach to promote school attendance (PCC, n.d.; Taylor et al., 2011; Fisher, 2008).
Conclusion
Chronic absenteeism is an indicator of both health and social needs in middle school-aged children and their families and may offer a snapshot of overall child health. Chronic absenteeism is associated with poor health and reduced developmental potential and is a vital sign that could benefit from monitoring and management. Strengths of this indicator include a uniform operational definition and widespread use as a school accountability metric. However, the potential mismatch between geographies for which the measure is typically available and the geography of health care system catchment area is a current limitation. Moreover, the meaning of chronic absenteeism may shift over the next several years as some students opt to learn virtually even after the COVID-19 pandemic recedes. Further development of chronic absenteeism as a potential health system performance measure could allow the impact of collaboration between education and health systems to be systematically monitored. The short- and long-term impacts of changes in school attendance for child, family, and community health may ultimately manifest in meaningful changes in educational attainment and population well-being, in addition to more traditional measures of disease prevalence and severity, preventive and acute care utilization, and cost.
Looking forward, chronic absenteeism may take on renewed importance as a vital sign as the U.S. works to recover from the health, economic, social, and educational impacts of the prolonged COVID-19 pandemic. Health systems can play a key role in anticipating and supporting student and staff psychosocial and health needs—for example, creating population-health oriented relationships between health systems and schools to increase access to mental and behavioral health services, or promote the capacity of school health and educational staff to address mental and behavioral health concerns. Even as schools across the country return to full implementation of in-person learning, barriers to attendance at the student, family, and school levels are likely to persist in the absence of focused attention to and remediation of chronic absenteeism. Chronic absenteeism in school-age children may offer a valuable indicator with which to monitor the success of efforts to promote child health and academic success over time.
Join the conversation!
![]() Tweet this! “Measuring students’ chronic absenteeism may provide an indicator of the adequacy of interventions to promote health and educational equity at the population level.” Read more in a new #NAMPerspectives: https://doi.org/10.31478/202306c
Tweet this! “Measuring students’ chronic absenteeism may provide an indicator of the adequacy of interventions to promote health and educational equity at the population level.” Read more in a new #NAMPerspectives: https://doi.org/10.31478/202306c
![]() Tweet this! Authors of a new #NAMPerspectives describe the importance of measuring chronic absenteeism to understand children’s health and health disparities. Read more at: https://doi.org/10.31478/202306c
Tweet this! Authors of a new #NAMPerspectives describe the importance of measuring chronic absenteeism to understand children’s health and health disparities. Read more at: https://doi.org/10.31478/202306c
Download the graphic below and share on social media!

References
- Allensworth, E. M., and J. Q. Easton. 2007. What matters for staying on-track and graduating in Chicago public schools. UChicago Consortium on School Research. Available at: https://consortium.uchicago.edu/publications/what-matters-staying-track-and-graduating-chicago-public-schools (accessed February 15, 2023).
- Allison, M. A., E. Attisha, Council on School Health, M. Lerner, C. D. De Pinto, N. S. Beers, E. J. Gibson, P. Gorski, C. Kjolhede, S. C. O’Leary, H. Schumacher, and A. Weiss-Harrison. 2019. The link between school attendance and good health. Pediatrics 143(2). https://doi.org/10.1542/peds.2018-3648.
- Ambrose, A. J. H. 2020. Inequities during COVID-19. Pediatrics 146(2). https://doi.org/10.1542/peds.2020-1501.
- Attendance Works. 2020a. Monitoring attendance in the 2021-22 school year. Available at: https://www.attendanceworks.org/chronic-absence/addressing-chronic-absence/monitoring-attendance-in-distance-learning/ (accessed February 15, 2023).
- Attendance Works. 2020b. The urgent need to avoid punitive responses to poor attendance. Available at: https://www.attendanceworks.org/the-urgent-need-to-avoid-punitive-responses-to-poor-attendance/ (accessed February 15, 2023).
- Attendance Works. 2018. Chronic absence. Available at: https://www.attendanceworks.org/chronic-absence/the-problem/ (accessed February 15, 2023).
- Attendance Works and Everyone Graduates Center. 2021. Using chronic absence to map interrupted schooling, instructional loss, and educational inequity: Insights from school year 2017-18 data. Available at: https://www.attendanceworks.org/wp-content/uploads/2019/06/Attendance-Works-Using-Chronic-Absence-to-Map_020221.pdf (accessed April 13, 2023).
- Balfanz, R., and V. Byrnes. 2012. Chronic absenteeism: Summarizing what we know from nationally available data. Johns Hopkins University Center for Social Organization of Schools. Available at: https://ccrscenter.org/products-resources/resource-database/chronic-absenteeism-summarizing-what-we-know-nationally (accessed February 15, 2023).
- Balfanz, R., L. Herzog, and D. J. Mac Iver. 2007. Preventing student disengagement and keeping students on the graduation path in urban middle-grades schools: Early identification and effective interventions. Educational Psychologist 42(4):223–235. Available at: https://new.every1graduates.org/wp-content/uploads/2012/03/preventing_student_disengagement.pdf (accessed February 15, 2023).
- Baltimore Education Research Consortium (BERC). 2011. Destination graduation: Sixth grade early warning indicators for Baltimore city schools: Their prevalence and impact. Available at: http://baltimore-berc.org/pdfs/SixthGradeEWIFullReport.pdf (accessed May 15, 2023).
- Basch, C. E. 2011. Healthier students are better learners: A missing link in school reforms to close the achievement gap. Journal of School Health 81(10):593–598. https://doi.org/10.1111/j.1746-1561.2011.00632.x.
- Bauer, L., P. Liu, D. Schanzenback, and J. Shambaugh. 2018. Reducing chronic absenteeism under the Every Student Succeeds Act. Brookings, April 15. Available at: https://www.brookings.edu/research/reducing-chronic-absenteeism-under-the-every-student-succeeds-act/ (accessed May 15, 2023).
- Bruner, C., A. Discher, and H. Chang. 2011. Chronic elementary absenteeism: A problem hidden in plain sight. Attendance Works and the Child & Family Policy Center. Available at: https://www.attendanceworks.org/wp-content/uploads/2017/04/Chronic-Elementary-Absenteeism-A-Problem-Hidden-in-Plain-Sight.pdf (accessed May 15, 2023).
- Centers for Disease Control and Prevention (CDC). 2022. Children’s mental health. Available at: https://www.cdc.gov/childrensmentalhealth/index.html?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fmentalhealth%2Fstress-coping%2Fparental-resources%2Findex.html (accessed April 27, 2023).
- CDC. 2020. Reduce chronic school absence among early adolescents — AH‑07. Healthy People 2030. Available at: https://health.gov/healthypeople/objectives-and-data/browse-objectives/adolescents/reduce-chronic-school-absence-among-early-adolescents-ah-07 (accessed May 15, 2023).
- Chang, H. N., K. Gee, B. Hennessy, D. Alexandra, and A. Gopalakrishnan. 2021. Chronic absence patterns and prediction during COVID-19: Insights from Connecticut. Attendance Works. Available at: https://www.attendanceworks.org/wp-content/uploads/2019/06/Chronic-Absence-in-CT_011222.pdf (accessed April 13, 2023).
- Chang, H. N., L. Bauer, and V. Byrnes. 2018. Data matters: Using chronic absence to accelerate action for student success. Attendance Works. Available at: https://www.attendanceworks.org/data-matters/ (accessed May 15, 2023).
- Chang, H. N., and M. Romero. 2008. Present, engaged and accounted for: The critical importance of addressing chronic absence in the early grades. National Center for Children in Poverty. Available at: http://www.nccp.org/wp-content/uploads/2008/09/text_837.pdf (accessed May 15, 2023).
- Connolly, F., and L. S. Olson. 2012. Early elementary performance and attendance in Baltimore City schools’ pre-kindergarten and kindergarten. Baltimore Education Research Consortium, March 1. Available at: https://baltimore-berc.org/early-elementary-performance/ (accessed May 16, 2023).
- Cutler, D., and A. Lleras-Muney. 2006. Education and health: Evaluating theories and evidence. National Bureau of Economic Research. https://doi.org/10.3386/w12352.
- Eaton, D. K., N. Brener and L. K. Kann. 2008. Associations of health risk behaviors with school absenteeism. Does having permission for the absence make a difference? Journal of School Health 78(4): 223–229. https://doi.org/10.1111/j.1746-1561.2008.00290.x.
- Educators for Excellence. 2020. Voices from the virtual classroom: A survey of America’s teachers on COVID-19-related education issues. Available at: https://e4e.org/sites/default/files/voices_from_the_virtual_classroom_2020.pdf (accessed May 16, 2023).
- Fisher, E. S. 2008. Building a medical neighborhood for the medical home. New England Journal of Medicine 359(12): 1202–1205. https://doi.org/10.1056%2FNEJMp0806233.
- Forrest, C. B., K. B. Bevans, A. W. Riley, R. Crespo and T. A. Louis. 2011. School outcomes of children with special health care needs. Pediatrics 128(2): 303–312. https://doi.org/10.1542/peds.2010-3347.
- Goudeau, S., C. Sanrey, A. Stanczak, A. Manstead, and C. Darnon. 2021. Why lockdown and distance learning during the COVID-19 pandemic are likely to increase the social class achievement gap. Nature Human Behavior 5(10): 1273–1281. https://doi.org/10.1038/s41562-021-01212-7.
- Guttmacher, S., B. C. Weitzman, F. Kapadia, and S. L. Weinberg. 2002. Classroom-based surveys of adolescent risk-taking behaviors: reducing the bias of absenteeism. American Journal of Public Health 92(2): 235–237. https://doi.org/10.2105/ajph.92.2.235.
- Hallfors, D., J. L. Vevea, B. Iritani, H. Cho, S. Khatapoush, and L. Saxe. 2002. Truancy, grade point average, and sexual activity: A meta-analysis of risk indicators for youth substance use. Journal of School Health 72(5): 205–211. https://doi.org/10.1111/j.1746-1561.2002.tb06548.x.
- Hoagwood, K., D. Klein Walker, A. Edwards, J. W. Kaminski, K. J. Kelleher, J. Spandorfer, and E. G. Fox. 2023. Vital Signs for Pediatric Health: High School Graduation. NAM Perspectives. Discussion Paper, National Academy of Medicine, Washington, DC. https://doi.org/10.31478/202306d.
- Ingul, J. M., C. A. Klöckner, W. K. Silverman, and H. M. Nordahl. 2012. Adolescent school absenteeism: modelling social and individual risk factors. Child and Adolescent Mental Health 17(2): 93–100. https://doi.org/10.1111/j.1475-3588.2011.00615.x.
- Institute of Medicine (IOM). 2015. Vital Signs: Core Metrics for Health and Health Care Progress. Washington, DC: The National Academies Press. https://doi.org/10.17226/19402.
- Jacob, B. A., and K. Lovett. 2017. Chronic absenteeism: An old problem in search of new answers. Brookings, July 27. Available at: https://www.brookings.edu/research/chronic-absenteeism-an-old-problem-in-search-of-new-answers/ (accessed May 16, 2023).
- Jones, R., P. Hoare, R. Elton, Z. Dunhill, and M. Sharpe. 2009. Frequent medical absences in secondary school students: survey and case-control study. Archives of Disease in Childhood 94(10): 763–767. https://doi.org/10.1136/adc.2008.140962.
- Jordan, P., and R. Miller. 2017. Who’s in: Chronic absenteeism under ESSA. FutureEd. Available at: https://www.future-ed.org/whos-in-chronic-absenteeism-under-the-every-student-succeeds-act/ (accessed May 16, 2023).
- Kieffer, M. J., W. H. Marinell, and N. S. Stephenson. 2011. The middle grades student transitions study: Navigating the middle grades and preparing students for high school graduation. The Research Alliance for New York City Schools. Available at: https://steinhardt.nyu.edu/sites/default/files/2021-01/NavigatingMiddleGrades_2011.pdf (accessed May 16, 2023).
- Lai, J., and N. O. Widmar. 2020. Revisiting the digital divide in the COVID-19 era. Applied Economic Perspectives and Policy 43(1): 458–464. https://doi.org/10.1002/aepp.13104.
- Lara, J., K. Nobel, S. Pelika, and A. Coons. 2018. Chronic Absenteeism. NEA Research Brief. NBI No. 57. National Education Association. Available at: https://eric.ed.gov/?id=ED595241 (accessed May 16, 2023).
- Lee, J. O., R. Kosterman, T. M. Jones, T. I. Herrenkohl, I. C. Rhew, R. F. Catalano and J. D. Hawkins. 2016. Mechanisms linking high school graduation to health disparities in young adulthood: a longitudinal analysis of the role of health behaviours, psychosocial stressors, and health insurance. Public Health 139: 61–69. https://doi.org/10.1016/j.puhe.2016.06.010.
- Lockee, B. B. 2021. Online education in the post-COVID era. Nature Electronics 4(5–6). https://doi.org/10.1038/s41928-020-00534-0.
- Musser, M. P. 2011. Taking attendance seriously: How school absences undermine student and school performance in New York City. The Campaign for Fiscal Equity. Available at: http://graphics8.nytimes.com/packages/pdf/nyregion/20110617attendancereport.pdf (accessed May 16, 2023).
- National Academies of Sciences, Engineering, and Medicine (NASEM). 2019. School Success: An Opportunity for Population Health: Proceedings of a Workshop—in Brief. Washington, DC: The National Academies Press. https://doi.org/10.17226/25370.
- Public Health Informatics Institute (PHII). 2020. Summary of laws related to child and adolescent mental health. Available at: https://phii.org/wp-content/uploads/2020/08/Summary-of-Laws-Related-to-CAMH.pdf (accessed February 16, 2023).
- Primary Care Collaborative (PCC). n.d. Medical neighborhood. Available at: https://www.pcpcc.org/content/medical-neighborhood (accessed February 19, 2023).
- Reich, J., C. J. Buttimer, A. Fang, G. Hillaire, K. Hirsch, L. Larke, J. Littenberg-Tobias, R. Moussapour, A. Napier, M. Thompson, and R. Slama. 2020. Remote learning guidance from state education agencies during the COVID-19 pandemic: A first look. EdArXiv Preprints. https://doi.org/10.35542/osf.io/437e2.
- Robert Wood Johnson Foundation (RWJF). 2016. The relationship between school attendance and health. Health Policy Snapshot. Available at: https://files.eric.ed.gov/fulltext/ED592870.pdf (accessed February 19, 2023).
- Rogers, T., and A. Feller. 2016. Reducing student absences at scale by targeting parents’ misbeliefs. Nature Human Behaviour 2: 335–342. https://doi.org/10.1038/s41562-018-0328-1.
- Schanzenbach, D. W., L. Bauer, and M. Mumford. 2016. Lessons for broadening school accountability under the Every Student Succeeds Act. The Hamilton Project. Available at: https://www.hamiltonproject.org/assets/files/lessons_broadening_school_accountability_essa.pdf (accessed May 16, 2023).
- Taylor, E. F., T. Lake, J. Nysenbaum, G. Peterson, and D. Meyers. 2011. Coordinating care in the medical neighborhood: Critial components and available mechanisms. Agency for Healthcare Research and Quality. Available at: https://www.ahrq.gov/sites/default/files/wysiwyg/ncepcr/tools/PCMH/coordinating-care-in-the-medical-neighborhood-white-paper.pdf (accessed February 19, 2023).
- U.S. Department of Education (DOE). 2023. The EDFacts Initiative. Available at: https://www2.ed.gov/about/inits/ed/edfacts/index.html (accessed February 15, 2023).
- DOE. 2019. Chronic absenteeism in the nation’s schools: A hidden educational crisis. Available at: https://www2.ed.gov/datastory/chronicabsenteeism.html#intro (accessed May 16, 2023).
- U.S. Department of Education Civil Rights Data Collection (DOE CRDC). 2019. 2017–18 CRDC data. Available at: https://www2.ed.gov/about/offices/list/ocr/docs/crdc-2017-18.html (accessed April 13, 2023).
- DOE CRDC. 2018. Wide-ranging education access and equity data collected from our nation’s public schools. Available at: https://ocrdata.ed.gov/ (accessed May 16, 2023).
- Weathers, E. S., K. B. Hollett, Z. R. Mandel, and C. Rickert. 2021. Absence unexcused: A systematic review on truancy. Peabody Journal of Education 96(5): 540–564. https://doi.org/10.1080/0161956X.2021.1991696.
- Wood, J. J., S. D. Lynne-Landsman, D. A. Langer, P. A. Wood, S. L. Clark, J. M. Eddy and N. Ialongo. 2012. School attendance problems and youth psychopathology: Structural cross-lagged regression models in three longitudinal data sets. Child Development 83(1): 351–366. https://doi.org/10.1111/j.1467-8624.2011.01677.x.
