Background Information
Physician-scientists are essential to bridging research and patient care. However, these unique professionals face mounting challenges, including unstable funding, prolonged training timelines, limited institutional support, and competing clinical and research demands that threaten the viability of this critical career path. With this context, the National Academy of Medicine (NAM), together with the American Junior Investigator Association (AJIA), hosted a workshop in September 2025 titled “Sustaining the Biomedical Workforce: Innovative Pathways for Retaining and Supporting Physician-Scientists” (see Box 1 for a list of workshop planning committee members and Box 2 for a list of speakers and moderators).
This workshop convened leaders from academia, government, industry, philanthropy, and health systems to confront long-standing structural challenges and explore bold, innovative models for sustaining physician-scientist careers. Through retrospective analysis, forward-looking panels, and solution-driven breakout sessions, participants sought to co-develop actionable strategies to support and retain this critical segment of the biomedical workforce.
Meeting Summary
Context and Framing
Physician-scientists make up just 1.3 percent of the physician population in the United States today, said Dr. Jennifer Kwan, AJIA and Yale University, and those in early stages of their career are the most vulnerable in the pipeline. While many stakeholders and reports have called for strengthening the US biomedical research workforce, challenges such as grant uncertainty, clinical demands, and misaligned incentives all contribute to the decline of physician-scientists conducting research (Kwan and Gross, 2023). She shared survey data collected in summer 2024, reporting that 49 percent of respondents (n=260) had considered leaving their career (Farhat et al., 2025). Top reasons for leaving included unhappiness, stress and burnout, undercompensation, and funding challenges. With these statistics as the backdrop, Dr. Kwan underscored the need to find bold solutions and identify opportunities for change that can effectively improve the system supporting this workforce.
The Importance of Recruiting Physician-Scientists
Dr. Robert Lefkowitz, Duke University, reflected on his formative years as part of the cohort of young physicians conscripted into the US Public Health Service during the Vietnam War and assigned to the National Institutes of Health (NIH). He described the Berry Plan, which allowed physicians to defer obligatory military service until they had completed residency, and then serve in the Army, Navy, Air Force, or US Public Health Service. Unlike the Army, Navy, or Air Force, participation in Public Health Service opportunities meant assignment to NIH or the Centers for Disease Control and Prevention rather than deployment to Vietnam. This made such commissions extraordinarily competitive—of thousands of annual medical graduates, fewer than 10 percent secured positions at NIH. Those select few were formally known as Clinical Associates under the Associate Training Program but informally became regarded as the “Yellow Berets,” a tongue-in-cheek contrast to the elite Green Berets. Dr. Lefkowitz said that at the time, he had not done any research and only intended to pursue clinical practice. But the draft redirected him, and although his first year of research was difficult, eventually he was able to publish his first papers, setting him on a scientific path.
The Associate Training Program’s design, he explained, was uniquely conducive to producing leaders in academic medicine. Laboratories and patient wards were physically adjacent to one another, encouraging translational thinking even among basic scientists. He also emphasized the importance of basic science being at the core of medical education, so that there was bidirectional understanding between basic science and clinical medicine. The results were extraordinary, said Dr. Lefkowitz. By the 1990s, 15–30 percent of chairs and deans at major institutions were former Yellow Berets. By 2010, 64 Yellow Berets had been elected to the National Academy of Sciences and 125 to the Institute of Medicine (now the National Academy of Medicine), and four became NIH directors (Khot et al., 2011). His own 1968 class encompassed individuals responsible for discoveries ranging from statins to a family of receptors that now serve as targets for one-third of all FDA-approved drugs.
Dr. Lefkowitz stressed the role of mentorship in this field, showing a diagram of how many different Nobel laureates were connected through scientific “lineages” of trainees and mentors. He noted how many laureates were physicians first, emphasizing the contributions of physician-scientists who bridged patient care with discovery science. But the landscape of medical education has shifted over the past 60 years, he added. For example, there is no doctor draft nor any service obligation for young adults anymore, and basic science is no longer at the core of medical education—often restricted to just one year or less. There are also few scientifically oriented faculty in clinical departments who could serve as role models. Last, he argued that it is no longer a widely held belief that understanding physiology is fundamental to progress in medicine.
Translating these lessons to the challenges of today, Dr. Lefkowitz proposed several ideas to overcome this gap in the workforce. First, he suggested medical schools adopt new models of curricula that place greater emphasis on rigorous basic science training and meaningful laboratory exposure, while stressing the scientific and experimental foundations underlying the current understanding of physiology and therapeutics. Building on his Yellow Beret experience, he also outlined the possibility of developing government-supported peacetime service programs for physicians in training that would be highly competitive, prestigious, and rooted in strong mentorship. Last, he advocated for greater inclusion of physician-scientists as role models in clinical training, so that students can see this dual path in action.
Sustaining Physician-Scientists in Biomedical Research
In his keynote address, Dr. Jay Bhattacharya, NIH, highlighted the critical challenges facing early-career researchers, adding that this is not a new problem, but one that goes back decades. He presented data illustrating some of the barriers to independence for physician-scientists. For example, in 1981, first Research Project (R01) awards were often secured while investigators were still in their thirties. Today, this funding award is not typically achieved until researchers are in their forties (see Figure 1). Similarly, attrition in early-career fellows has also risen from about 15 percent of Postdoctoral Individual National Research Service Award (F32) fellowship recipients leaving the research pipeline within a few years, to more than 50 percent dropping out now. Dr. Bhattacharya emphasized that the current scientific infrastructure makes it increasingly difficult for young researchers to test new ideas, creating a system that effectively “advances science one obituary at a time.” However, studies have found that younger researchers are more likely to introduce and work with novel, more innovative ideas. Echoing Dr. Lefkowitz, Dr. Bhattacharya highlighted the vital role of mentorship and the potential for pairing early-career first authors with more senior investigators.
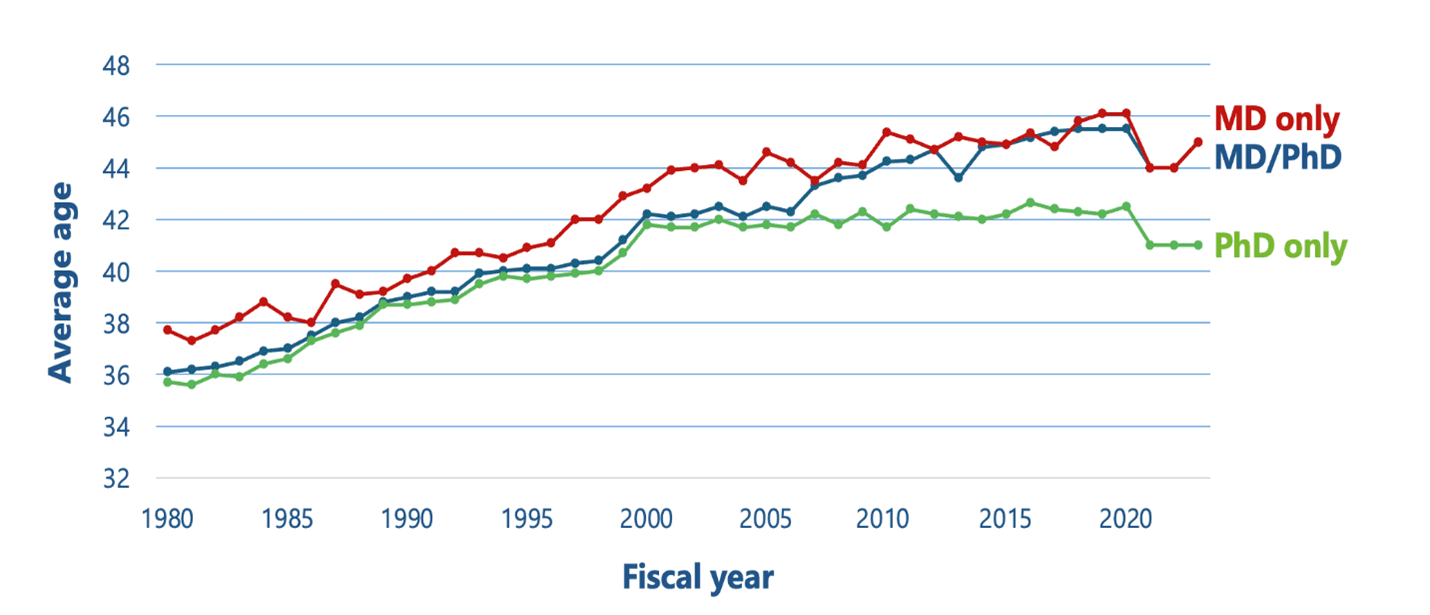
Figure 1 | Average Age of First Time R01 Recipients (1980–2023)
SOURCE: Bhattacharya presentation at the Sustaining the Biomedical Workforce joint workshop from the AJIA and the NAM. September 9, 2025. Available at: https://nam.edu/event/sustaining-the-biomedical-workforce-innovative-pathways-for-retaining-and-supporting-physician-scientists/ (accessed March 25, 2026).
Dr. Bhattacharya outlined several structural challenges that hinder the advancement of innovative science within the biomedical research ecosystem. First, he noted that the current biomedical research ecosystem punishes failure too harshly—unlike the culture of Silicon Valley where failed ventures are part of the process and often used as “stepping stones” to success. This risk-averse culture undermines scientific advancement, he noted. Also related is the shift in grantmaking at the NIH, where he explained that grants in the 1980s were typically awarded to support ideas that were only a year or two old. But by the 2000s, the ideas awarded were, on average, already seven years old, reflecting a reluctance to support novel science (Packalen and Bhattacharya, 2020). This problem is compounded when looking at the age of researchers and the age of ideas. Generally, for every one year of chronological age, the age of the ideas in papers goes up by about one year (Packalen and Bhattacharya, 2019). We need a scientific infrastructure that allows early-career researchers to try out their new ideas, he said. The last challenge Dr. Bhattacharya outlined is the ongoing issue of public trust, as he shared that one in four Americans think that scientists do not act in the best interests of the public (Pew Research Center, 2023).
Dr. Bhattacharya proposed several reforms to address these challenges. First, he called for de-risking transformative research so that early-career scientists feel supported in exploring novel ideas without immediate pressure for success, and so that failures can be seen as constructive learning opportunities. Second, he emphasized the need for more comprehensive and nuanced metrics of scientific productivity that extend beyond simple counts of publications or citations. In this context, he pointed to steps NIH has taken to address some of these concerns, including efforts to centralize peer review, streamline review criteria to improve objectivity and consistency of evaluation, adopt a more flexible, portfolio-based grant funding policy that gives institute directors more flexibility to take risks, and expand institutional career development (K) awards. Overall, he closed with optimism that the biomedical research ecosystem receives strong bipartisan support but argued that a culture shift is needed to support the exploration of innovative thinking and new approaches.
Lessons from Past Efforts
The opening panel focused on national efforts to support physician-scientists, offering a candid assessment of what has and has not worked in the past. Speakers included Mr. Sam Gill, Doris Duke Foundation (DDF), Dr. Louis Muglia, Burroughs Wellcome Fund (BWF), Dr. David Ginsburg, University of Michigan, Dr. Mukesh Jain, Brown University, and Dr. Ivy Ng, Singapore Health Services Pte. Ltd. The panel was moderated by Dr. Juanita Merchant, University of Arizona.
Dr. Ginsburg shared insights from his perspective of the 2012 Physician-Scientist Working Group, noting that the most successful physician-scientists had significant research experiences as undergraduates and benefited from mentorship by attending physicians who were themselves active investigators. However, he observed that the training and practice environment has shifted significantly over the past decade, from one that more readily accommodated research engagement to one increasingly driven by clinical productivity. For example, health systems now prioritize clinical efficiency over research engagement, he explained, and clinicians are evaluated primarily on relative value units (RVUs), leaving less protected time and fewer incentives for research involvement. These elements contributed to lengthened training periods, increased specialization, and added administrative burden. Dr. Ginsburg recommended returning to historical mentorship models, strengthening basic science education, and creating pathways that better integrate clinical practice and research careers.
During his opening remarks, Dr. Jain reiterated similar points from others emphasizing support for physician-scientists, highlighting the importance of community and careful selection of mentors. Given the financial pressures of health care systems that have 1–2 percent operating margins, he suggested demonstrating the value of research to hospital leadership and board members—adding that research can also attract top talent and contribute to alternative revenue streams. He shared examples of institutions that have created a shared vision between medical schools and health systems to support physician-scientists, such as the University of California, Los Angeles (UCLA), the University of Pennsylvania, and Vanderbilt University.
Dr. Ng summarized Singapore’s experience in developing an academic health system, following the changes and new goals for biomedical research put forward in 2000. She explained that critical momentum came from a government task force that set a national vision for biomedical sciences, coupled with a tight partnership between SingHealth (the public health cluster) and Duke‑NUS Medical School. In 2005, Singapore established a second medical school in partnership with Duke University. With no dedicated resources initially for academic medicine, they implemented organizational restructuring, creating joint leadership teams and multi‑layered academic structures linking the school and health system, instituting clear academic performance metrics tied to incentives, and establishing a Centre for Clinician-Scientist+ Development and dedicated clinician‑scientist training pathways. She shared other strategies such as integrating research and clinical missions, leveraging mentorship schemes in place at Duke, and creating environments supportive of research. Outcomes were positive, said Dr. Ng, such as increasing the proportion of physician-scientists from just 1 percent to 10 percent. They also reduced attrition to private practice and supported the workforce pipeline through specialized clinician-scientist residency programs. She acknowledged that sustained funding continues to be a challenge but urged stakeholders to view physician-scientists as an “endangered species” that requires continuous nurturing.
As presidents of major philanthropies supporting physician-scientists, Mr. Gill and Dr. Muglia explained that their organizations have invested hundreds of millions over the past three decades, learning how best to change the paradigm. Mr. Gill explained that physician-scientists have historically driven outsized innovation. Over 25 years, DDF invested approximately $320 million in support for physician-scientists but has seen mixed results. Through different funding mechanisms, the organization learned that brief research exposure for medical students led to just single-digit percentages of participants becoming career researchers. While they found flexible early-career support to be most effective in advancing research, he noted that it primarily helped to accelerate research progression and not as much novel research discovery. Mr. Gill described the struggle at DDF to change existing research paradigms and drive innovation in research, as well as their challenge to address inequality in representation among early-career researchers. Specifically, he highlighted the double-edged sword of social networks, saying they can be crucial for research success, but can also reinforce existing demographic patterns and systemic inequities. Dr. Muglia described a similar commitment to physician-scientists at BWF, recounting approximately $300 million of investment since 1993, with flexible awards designed to support risk-taking and build mentorship communities. Through various models and awards, BWF has been trying to address key challenges of protecting research time and creating more opportunities for community building and mentorship. Looking to the future, Dr. Muglia said they are seeking to support researchers before they are competitive for traditional awards, and that BWF’s awards will continue to prioritize diversity in the workforce.
Discussion
Throughout the discussion, speakers emphasized the importance of taking another look at program design and what is taught in medical schools. Planning committee member Dr. Vivian Cheung, Brown University, suggested that careful selection and intense mentorship can seed careers, and others added the possibility of cross-institutional mentoring. Speakers agreed on the need for more basic science in the curriculum and bringing the focus back to bedside, though various models for this exist. Dr. Robert Califf, Duke University, argued that current systems do not support fundamental, early-stage research and suggested a need for funding mechanisms that support exploratory research without immediate commercial potential.
As highlighted in the opening remarks, bandwidth and burnout continue to be a challenge for physician-scientists. A participant noted that many are simply overburdened by their clinical, compliance, and research obligations. Dr. Jain acknowledged the load, especially related to regulatory and certification compliance and advocated for improvement. Other suggestions to alleviate burnout included reducing administrative burdens and RVU pressure by creating more flexible evaluation metrics. Using explicit mechanisms for protected research time that still emphasize community building and mentoring can also help ensure physician-scientists are not overwhelmed by their obligations. As an example, a participant noted that the US Department of Veterans Affairs system provides flexibility in clinical demands and has a less strict RVU-driven environment that could be built on.
Timing to career independence was also discussed as a challenge. Lack of interest in a physician-scientist career is not the issue, but the extended time to independence and limited post-training support available to trainees present challenges. Other attendees similarly called for shortened training and increased investment in discovery research.
Physician-Scientists in an Evolving World of Science and Technology
A subsequent panel focused on the evolving identity of physician-scientists and their critical role in accelerating the translation of discovery into improved health outcomes. Topics highlighted integrating digital health and entrepreneurial models, advancing team science, and strengthening training pathways. Speakers included Dr. Elena Fuentes-Afflick, Association of American Medical Colleges (AAMC); Dr. Robert Califf, Duke University; Dr. Anna Greka, Harvard University, Mass General Brigham, and Broad Institute of Massachusetts Institute of Technology and Harvard University; Dr. Kenneth Mandl, Boston Children’s Hospital and Harvard Medical School; and Dr. John Sampson, University of Colorado Anschutz School of Medicine. The panel was moderated by Dr. Joseph Wu, Stanford University.
Dr. Fuentes-Afflick framed her remarks by sharing recent data from several different surveys related to physician-scientists. A 2025 AAMC survey found that 90 percent of students reported participation in a faculty-mentored research project, and about half planned to do research in their careers, but just 3 percent planned to focus on research exclusively (AAMC, 2025). A 2022 AAMC National Sample Survey of Physicians found that 14 percent engaged in research, with almost 4 percent of this group devoting more than half of their time to research and 84 percent spending no more than 10 percent of their time on research (Browne, 2024). Looking forward, Dr. Fuentes-Afflick highlighted several priorities, including funding and training stability, using broader definitions (e.g., “research-engaged physicians”), and putting resources toward institutional supports—including mentorship, networks, and team-science structures—while also seeing artificial intelligence (AI) as a cross-cutting capability rather than a replacement for those foundations.
Dr. Califf challenged the distinction of “industry vs. academia” and argued that health care delivery is, in itself, an industry with far greater money and power than the medical products sector. He called attention to the design of the current system, which often prioritizes financial optimization over research and learning opportunities. There is a need for a shift to a learning health system dedicated to continuous improvement, knowledge generation, and patient outcomes, he said. Currently, even retail industries are using data more effectively for improvement, and health care should follow suit, he said. Dr. Califf argued for a fundamental restructuring of the health care ecosystem, breaking down silos between research, clinical practice, and different sectors involved in health care delivery, and rebuilding in an integrated manner so that everyone would be dedicated to learning for better patient outcomes rather than financial optimization.
Dr. Greka shared the diversified model of the Broad Institute, a nonprofit research center focused on genomics and biomedical research. Approximately one-third of their budget comes from federal money, one-third from philanthropy, and one-third from industry. She stressed philanthropy’s role in seeding high-risk ideas before they capture attention from NIH or industry—which is a playbook the physician-scientist ecosystem can emulate. As an American Society for Clinical Investigation (ASCI) leader, Dr. Greka highlighted early-career retention programs such as the Emerging-Generation Awards and Young Physician-Scientist Awards, which establish mentorship connections, and Mentored Clinical Scientist Development Awards (K08) cohorts, which create buddy networks and track success. As potential ways to address the “leaky” nature of the workforce pipeline, Dr. Greka discussed the new ASCI Impact Fund with the goal of permanently endowing early-career programs, as well as their goals of developing partnerships with industry and philanthropy to increase funding support for physician-scientists.
Dr. Mandl focused on the role of physician-scientists in the evolving digital age, highlighting the changing landscape and the potential for AI to assist in delivering health care more broadly—so it is becoming increasingly important to have relevant AI skills and the ability to incorporate them into research and health care delivery. Effective precision medicine and use of AI require blurring the lines between research, clinical practice, and technology. There are potential new career paths, he noted, with future physician-scientists having computer science backgrounds or AI PhDs not needing traditional MD training to understand clinical domains. But challenges in funding, regulation, and industry relationships will still present barriers, and he emphasized the need for interdisciplinary approaches and—reiterating comments from others—blending research and clinical domains.
Dr. Sampson shared his perspective as a surgeon-scientist, saying that as a group, surgeon-scientists are not inherently disadvantaged in academic medicine but can be quite profitable for hospitals and may even have unique opportunities to leverage philanthropic support. But he also criticized the lengthy medical training required to be a surgeon-scientist, especially in the age of AI, and argued for more merit-based approaches to medical education. He also noted that although current systems systematically undervalue physician-scientists, looking at balance sheets within a health system, even if they have thin margins, the money exists. Still, there is a need for fundamental restructuring of how physician-scientists are supported and compensated. Dr. Sampson called for changing the model, saying that health systems are not set up to value learning and research, and therefore are missing opportunities to improve the system and reduce costs.
Discussion
During the discussion portion of the workshop, speakers commented on the attractiveness of the field and the potential for rebranding physician-scientist careers as exciting engines of discovery, reproducibility, and implementation. Dr. Sampson added that while it may be difficult to compete with the novelty of emerging fields like AI and startup opportunities, branding the importance of “patient impact” can be a meaningful selling point for physician-scientist candidates.
Part of this challenge also includes the financial considerations and career commitment for research, where grant deadlines may require working on weekends or giving up leisure time that clinicians would get to enjoy. Dr. Wu argued that these considerations play a crucial role in career decisions and urged institutional leaders to solve these persistent compensation and support issues so that talented candidates do not have to walk away from a research career. There are already workforce shortage concerns, with one report estimating that 1,000 individuals will need to enter the pipeline every year just to maintain a steady state (NIH, 2014). Dr. Sampson and Dr. Califf also argued for system-level solutions and better storytelling about the importance of physician-scientist careers and the societal returns on investment. In response to a question about research that does not generate clear return on investment, Dr. Califf noted that non‑market public and philanthropic funding is essential for basic discovery research. Last, participants emphasized broadening the definition of “physician-scientist” beyond traditional bench lab research to include those who study health economics, policy, and population sciences or conduct clinical trials. This in turn broadens the value and impact of the physician-scientist population.
Bold Models for Sustainable Support
The third panel reviewed innovative domestic and global models for sustaining physician-scientist careers, examining state-driven initiatives, mission-oriented and public-private funding strategies, the role of philanthropy and venture capital, and emerging synergies between health systems and universities. Speakers included Dr. PJ Utz, Stanford University, Dr. Michelle Le Beau, Cancer Prevention Research Institute of Texas (CPRIT) and University of Chicago, Dr. Carole Jabet, Fonds de Recherche du Québec (FRQ), and Dr. Say Beng Tan, Singapore National Medical Research Council (NMRC). The panel was moderated by Dr. Vivian Lee, Harvard Business School.
Dr. Utz suggested viewing the “pipeline” metaphor instead as a “refinery,” as it is not linear but rather a more complex process with multiple stages of development and refinement. There are many touchpoints from pre-collegiate education to postdoc years to independence, where individuals are refined along the way. He warned of fragility in multiple areas of the refinery, including waning STEM culture in elementary and secondary schooling in the United States, especially compared to peer countries like China and Japan. He recounted some of the challenges he has experienced related to sustainable funding. For example, last year Stanford saw a 3 percent decrease in slots for their Medical Scientist Training Program, a number expected to drop by another 10–15 percent this year across 34 MD-PhD programs. He proposed several solutions, including developing national high school research programs, supporting undergraduate opportunities, and developing innovative curriculum models. He outlined Stanford’s five-year split curriculum, where the first year is standard medical school and subsequent years allow significant research time. Dr. Utz emphasized the importance of integrating different training steps but also called for broadening the definition of success beyond just securing R01 grants.
Dr. Le Beau described the state-based model at CPRIT, created in 2007 by a Texas constitutional amendment. With $3 billion authorized in initial commitment, she explained it was renewed to $6 billion in 2019, with an annual budget of $300 million. CPRIT has invested resources across more than 2,100 grants to date, spanning academic research, product development, and prevention. While they have recruited 340 investigators, only 17 percent are MDs or MD-PhDs, she said, and this is heavily weighted toward senior, more established investigators. Recounting lessons learned, Dr. Le Beau noted that state-based initiatives can have a very high return on investment, leading to other benefits for the state, including business growth, academic growth, and biotech development. The legislature also mandates that institutions receiving awards match 50 percent of the funds, which can help build sustainability of efforts. She shared that CPRIT experienced some of the complexity of public-private partnerships, especially around intellectual property terms and indirect cost limitations, requiring close coordination with partner institutions. Overall, Dr. Le Beau emphasized that carefully designed state-level funding can be a powerful mechanism for driving research innovation and supporting scientific development, particularly when aligned closely with institutional and regional needs.
Dr. Jabet shared the mission of FRQ as a Canadian governmental agency to support research capacity in the academic sector. Financed through provincial funding, the Ministry of Economy and Health, and the Federation of Medical Specialists of Québec, the FRQ budget focuses on supporting research careers (with 38 percent of grants going to physician-scientists), training programs, and research operations in health care organizations and hospitals. The physician-scientist career pathway funds research across all pillars (clinical, epidemiological, basic research), pairing protected time and mentorship with a salary model that eliminates the pay gap. FRQ funds the protected time for research, and the Federation of Medical Specialists contributes additional funds so a physician-scientist “earns the same as a full-clinical peer,” Dr. Jabet explained. FRQ’s unique funding model supports physician-scientists for 12–15 years, but challenges remain in supporting them throughout their careers. Additionally, the government-controlled health care system limits physician numbers, and similar to other organizations, there is increasing pressure to focus solely on clinical work—impacting protected research time.
Dr. Tan presented Singapore’s approach to supporting physician-scientists in a tightly coordinated national system. Singapore has three integrated regional health care clusters, offering full health care services, three medical schools, and multiple research funding agencies. Project grants do not cover an investigator’s salary; hospitals pay for that clinical work. Therefore, to avoid a mismatch, NMRC created competitive awards that buy out clinician time, so the investigator can spend a specified portion of their time on research instead of clinical duties. Through this salary support, they can protect research time for physician-scientists and create awards that incentivize different research approaches across various career stages. While NMRC still encounters challenges such as a high clinical workload, sustainability of funding, and developing talent in emerging areas like AI, they have also experienced many signs of success. Dr. Tan highlighted government support and recognition, close engagement between funders and institutions, willingness to adapt programs as needed, and public recognition of physician-scientists. Looking forward, Dr. Tan emphasized the importance of creating flexible mechanisms that recognize and enable physician-scientists to excel in their work across diverse research domains.
Discussion
During the panel discussion, speakers and participants highlighted important common themes among the various models presented. For example, several elements of funding and support models were mentioned, such as the evidence for return on investment and leveraging reinvestment. Dr. Le Beau said that CPRIT has demonstrated how to show value through job creation, cost savings (e.g., through cancer screening), patents, and company capital. Dr. Lee emphasized that universities have clinical insights and patient access that could be leveraged through industry partnerships to directly support physician-scientists and reinvest in intellectual property. Regarding salaries, Dr. Jabet noted the benefit of income security through FRQ’s equal pay policy, which prevents pay cuts and keeps physician-scientists at parity with their clinical peers. Summarizing the conversation, Dr. Victor Dzau, NAM, called for a scalable model for supporting physician-scientists that would demonstrate their value, equalize income between clinicians and scientists, provide long-term support, and include diversified sources of funding.
Lingering challenges persist, however, despite the success of various models, making adoption difficult. Dr. Tan and Dr. Jabet agreed that protected research time can be scarce, even with funding parity, as hospitals and health systems still prioritize clinical obligations over research. Dr. Utz added that the pipeline still needs fortifying, and without bold, early investments—such as high school and undergraduate exposure—the pool of future physician-scientists remains insufficient.
Designing Innovative Solutions
Following the panel presentations, the workshop shifted to five concurrent breakout sessions where participants could select the discussion most relevant to their background and expertise. To seed these discussions, a pre-event survey was sent to registrants to gather their perspectives and insights. Many themes from the survey reflect the discussions held at the workshop, including expanded metrics to better measure value and nuance, the need for strengthened mentorship programs, improved focus on core competencies in training, prioritization of decreased time to independence, integrated training, and even translation of skills to other sectors beyond research such as practice and policy. Specific suggestions from the survey for building support and momentum included protecting research time, creating endowed junior professorships, using public storytelling, and normalizing uncertainty.
This section outlines the key takeaways from the workshop breakout discussions, including challenges and potential solutions for each of the following topics: policy and communication, innovative funding mechanisms, redefining success and impact, retaining the pipeline, and novel paradigms for training.
Policy and Communication
Led by Dr. Yvette Seger, Federation of American Societies for Experimental Biology (FASEB), and Ms. Mary Woolley, Research!America, this breakout session focused on how to increase tangible support for physician-scientists through policy change, advocacy, and public engagement. Participants noted additional challenges in policy and communication, including the difficulties of advocating for any major policy reforms in the near term, given the unsettled federal environment and shifting NIH priorities. Current promotion of physician-scientists often depends on outdated or narrow success metrics and does not account for broader contributions, making it difficult for many. Within academic medical centers, leaders are hesitant to commit resources without stable external funding. Additionally, the group recognized that many physician-scientists and trainees want to engage with the public and policy makers, but do not have the advocacy and communication expertise. Communicating the value of physician-scientists remains difficult, as messages can risk sounding elitist or failing to resonate.
Several strategies were offered as potential solutions. At the policy level, participants called for pursuing multi-year federal funding commitments, while also encouraging state-level investment in biomedical research and workforce development, as seen at Texas’ CPRIT. Some suggested that physician-scientists should be more directly represented in governance, including nominating them to serve on the NIH Advisory Committee to the Director, and revisiting prior NIH working group recommendations. In terms of communications and advocacy, participants emphasized storytelling and reframing: highlighting relatable patient-centered narratives, framing physician-scientists as working “for you,” and portraying science as a process of “selling hope.” Partnering with patient advocacy groups was seen as a powerful way to increase impact, especially in district-level visits with members of Congress. Industry engagement was also highlighted, suggesting pharmaceutical and biotech partners could be allies in supporting training and development. Last, at the institutional level, participants called for academic medical centers to incorporate physician-scientist achievements into public communications and promotional campaigns, making their role more visible. Participants also noted that training in communication and advocacy skills should be integrated into medical education, responding to growing demands from trainees.
Physician-scientists need a new advocacy toolkit, said Dr. Seger, one that blends policy influence, patient partnerships, industry collaboration, and clear, hopeful messaging. By reframing their value narrative and making sure they are included in governance roles, physician-scientists can better sustain their careers and strengthen their impact on the nation’s health and innovation ecosystem.
Innovative Funding Mechanisms
The breakout discussion on innovative pathways, led by Dr. Ruben Flores-Saaib, Ligand Pharmaceuticals, explored alternative financing mechanisms and institutional strategies to sustain physician-scientist careers—especially during vulnerable transition periods like the K-to-R award funding gap. He invited perspectives on why venture capital (VC) investment is often cited as an alternative funding model. While VCs can provide funding for higher-risk projects or trainees working on translational projects, through a corporate entity subcontracting research, there is also a need to outline the structure of the investment up front when investing in people, as the long-term return on investment is not always clear.
The group discussed what types of financing could help ensure uninterrupted research time for investigators. One potential approach is through an endowed chair position for a junior investigator that changes each year. Additionally, linking clinical revenue to research, and potentially pooling money from high-performing clinical programs (e.g., cell therapy) could generate a stable internal system to allocate research funds where they are most needed.
To think about bridging funding and sustainable career pathways, a possible analogy could be to treat promising young investigators like sponsored athletes, with philanthropists or private companies providing early-career “endorsement” support. There are current examples where industry has sponsored fellows or considered sponsoring trainees as a “class” that could lead to the development of best practices for other companies to do the same. One participant emphasized that the most important asset is human capital and advocated for a better specific understanding of that value so it could be communicated more clearly.
While there is potential to reinvest financial gains from biomedical research to support physician-scientist development, participants noted the challenge in achieving this commitment. The group discussed “locking in” institutional reinvestment mechanisms—such as dedicating a fixed percent of the university share of royalties or licensing revenue to physician-scientist training. Participants emphasized that enshrining physician-scientist support in board-level policies, endowments, and royalty allocations can “lock in” commitments that make institutions more attractive to commercial and philanthropic partners. Setting this in stone can help to ensure stability across leadership transitions. While it can be difficult to control what happens everywhere, having best practice instructions on how to allocate money arising from commercial partners may help provide a guide for institutions and help standardize the practice across the field.
Redefining Success and Impact
Led by Dr. Olivier Elemento, Weill Cornell Medicine, this breakout session identified a critical challenge—the disconnect between narrow, institutionally-focused metrics and broader societal and personal definitions of success. Echoing previous comments, while metrics like measuring grants secured and papers published are entrenched in NIH reporting and academic promotion systems, they fail to capture the full range of contributions physician-scientists make to patient care, industry, policy, and broader society.
To address this in part, the group called for alternative metrics for promotion that recognize impact outside academic medical centers, such as leadership and mentorship roles, reputation and communication skills, team contribution, and application of training across sectors, not primarily by grants, publications, and citations. They also proposed incorporating “personal career satisfaction” as a legitimate metric of success for training programs, challenging the idea that only certain career paths are valid. Institutions could create physician-scientist–specific promotion tracks with clear and transparent criteria, ensuring fair recognition without punishing nonlinear careers.
The conversation offered some concrete mechanisms for recognizing contributions that are currently undervalued. Mentorship quality, not just quantity, should be assessed via 360-degree reviews. Changes should also be made to properly value team science. Participants suggested the traditional practice of first authors and last authors receiving recognition on papers needs to be amended, and multiple principal investigators (PIs) on grants should be treated as equivalent to that of a sole PI in review processes. Last, any data collected by institutions should be shared to ensure transparency in review and promotion processes, and to track whether changes are resulting in a more successful physician-scientist workforce.
There was also concern about unintended consequences when rethinking evaluations or using new or different tools. Seemingly helpful policies, such as extending the tenure clock, can backfire by delaying promotions and widening the gender gap in leadership. Similarly, requiring physician-scientists to manually collect data for new, broader metrics could create a system of “haves and have-nots” that would disproportionately burden already overtaxed individuals and reward those with the time, resources, and institutional knowledge. The group also advocated for clear, minimum criteria for promotion that guarantee advancement when met.
Retaining the Pipeline
Dr. Brendan Lee, Baylor College of Medicine, framed this session by noting the urgency of retaining physician-scientists across the training continuum, particularly in the face of increasing burnout. While there is still strong interest among trainees, structural disincentives and long, fragmented training pathways continue to challenge the pipeline. Critical bottlenecks in the pathway include K-to-R transitions, overextended training timelines, salary disparities, and lack of coordinated career support.
Reviewing the challenges in more detail, participants noted that attrition occurs at predictable transition points—most critically from K-to-R awards and from residency to fellowship, when financial pressures, long training times, and life responsibilities drive many out of research. MD-PhD physicians have a lower lifetime earning potential than MD physicians in the same specialty (Catenaccio et al., 2024). The length of training has also expanded significantly, reiterating points that faculty appointments that once came in one’s early thirties now often arrive in one’s mid-forties. Many MD-PhD trainees are also parents, which compounds the challenges of the extended duration of programs and stipend salary (Jansen et al., 2023). Hyper-competition has also inflated entry requirements: students now average multiple “gap years” and feel pressured to secure high-impact papers and career development funding before applying, which can delay independence. Participants also cited mentorship gaps, inconsistent compensation structures, and a lack of longitudinal data showing where trainees ultimately end up—making it hard to measure success or justify investment.
To address these vulnerabilities, participants argued for institutional reforms and, in some areas, targeted action from NIH. They called for shortening and linking training steps and creating linked funding mechanisms, such as structured F-to-K-to-R pathways, that bridge transitions for continuous support to help investigators across career stages. NIH could play a critical role in designing mechanisms, including revisiting past workforce task force recommendations, and evaluating outcomes of prior career development programs. A “supercharged award” such as the Pathway to Independence Award (K99/R00) was proposed to allow residents to carry portable funding and negotiate institutional offers. Other suggestions included separate funding pools for senior versus early investigators to avoid direct competition between them as well as scaling longer-duration Maximizing Investigators’ Research Award (R35) grants for better physician-scientist stability.
Although many are committed to the importance of the physician-scientist pipeline, without shortening the training timeline, greater financial sustainability, coordinated NIH and institutional investment, and recognition of diverse career trajectories, it will continue to erode. There is a broader need for institutions and federal partners to measure and demonstrate the economic value and reputational impact of their physician-scientist workforce to clarify the true return on investment.
Novel Paradigms for Training
This session, led by Dr. Linda Demer, UCLA, and Dr. Talia Swartz, Icahn School of Medicine at Mount Sinai, reiterated that talent and interest are not lacking in the field, but the long, rigid traditional pipeline is where the problem lies, misaligned with today’s scientific and clinical realities. To address this, speakers proposed embedding research experiences continuously within clinical training rather than extending training. Competency-based, not time-based, training models could allow earlier transitions to independence for those demonstrating readiness. Participants suggested advocacy and increased collaboration with accrediting bodies, such as the Accreditation Council for Graduate Medical Education (ACGME), and that specialty boards could encourage more flexible research time within residency programs. Some European models are designed so MDs can earn PhDs during later residency or early faculty years, allowing research continuity and smoother transitions to independent positions. Participants suggested integrating and aligning MD, PhD, and residency phases—through dual-credit coursework, coordinated committees, and residency research tracks to eliminate redundancy. Other proposals included early transition models, such as “Instructor + Startup” or hybrid faculty positions that give promising trainees lab resources and salary earlier to prevent attrition to private practice. A few cited successful models such as UCLA’s Specialty Training and Advanced Research (STAR) Program and the University of Pennsylvania’s physician-scientist pairing programs, where intensive mentoring with basic science leaders significantly shortened transitions.
Looking to the future needs of the workforce, cross-disciplinary competencies were emphasized, including data science and bioinformatics, entrepreneurship and innovation translation, leadership, fundraising, and communications. These skills are all essential for modern translational science. Thinking outside the box of typical training modalities, other models such as bootcamps, hackathons, or practicums can build these skills without extending the training timeline. While there will not be a one-size-fits-all model, programs like STAR, Stanford Biodesign, and Harvard’s Bioinformatics Graduate Certificate all present effective templates to build from.
Expanding physician-scientist training to include structured experiences outside traditional academic settings could strengthen both career sustainability and translational impact. Structured rotations or fellowships in industry, government, or other non-academic environments—even for limited periods—can help strengthen bidirectional translation. These experiences can also be facilitated through formal industry partnerships. For example, externships with biotech companies or regulatory agencies can help strengthen real-world problem solving and cross-sector collaboration. More broadly, institutions could formalize these collaborations through structured playbooks that address common issues such as human resources policies, data sharing, and intellectual property. These methods offer valuable exposure to product development, regulatory processes, and health system operations, while allowing trainees to bring clinical insight back to research. Importantly, these rotations should be time-limited, structured, partnership-based, and anchored in academic mentorship, so they function as skill-building experiences rather than recruitment pipelines.
Areas of Future Focus and Key Themes
Jennifer M. Kwan, Yale University; Victor J. Dzau, NAM; Evan K. Noch, University of Texas Southwestern Medical Center; Yvette R. Seger, FASEB; Mary Woolley, Research!America; Ruben D. Flores-Saaib, Ligand Pharmaceuticals; Andrew R. Zinn, University of Texas Southwestern Medical Center; Olivier Elemento, Weill Cornell Medicine; Brendan H. Lee, Baylor College of Medicine; Linda L. Demer, UCLA; and Talia H. Swartz, Icahn School of Medicine at Mount Sinai.
Based on the collective insights shared during the workshop discussions, the above-named individual authors believe that six key areas of action are most crucial to ensure a stronger biomedical workforce supporting physician-scientists, including:
Reimagining Education and Training Pathways
Current training pathways are lengthy, highly structured, and insufficiently integrated with real-world scientific practice and patient care. Multiple speakers urged medical schools to re-establish a strong foundational emphasis on basic science while moving toward competency-based, time-flexible training pathways. Participants also urged integrating research throughout clinical training rather than adding years to their timeline. Models such as Stanford’s five-year split curriculum, UCLA’s STAR Program, and Singapore’s competency-linked clinician-scientist programs could be used as prototypes. Shorter, integrated training that tolerates risk-taking, paired with necessary skills and competencies like data science, communication, and leadership, are important approaches to attracting and retaining talent. The utility of pre-doctoral gap years was also raised, with concerns that research accomplishments within these gap years often raise competitiveness for medical science training programs and feed a vicious cycle of more research time being needed for successful applicants. The Liaison Committee on Medical Education and ACGME could also act as partners in helping to shorten and modernize training requirements.
Building Sustainable and Diversified Funding Ecosystems
Across discussions, instability of funding was cited as one of the most critical barriers to building sustainable research ecosystems. Participants distinguished between two related but distinct challenges. First, the prolonged time to a first R01—now roughly a decade longer than in prior generations, as Dr. Bhattacharya noted—contributes to a “leaky pipeline” by delaying independence and making research careers less financially and professionally viable for early-career investigators. However, participants emphasized that funding instability more broadly also deters innovation: when success rates are low and renewals uncertain, investigators are incentivized to pursue safer, more fundable projects rather than high-risk, high-reward ideas. Moreover, a single R01 is often insufficient to sustain meaningful research effort, underscoring that time to first award alone does not fully explain the structural challenges facing innovation.
Participants pointed to potential solutions such as state-level initiatives (e.g., Texas CPRIT), salary parity models (e.g., Québec FRQ), national salary-buyout awards (e.g., Singapore NMRC), and industry partnerships. Multiple speakers emphasized the importance of blended funding across federal, state, institutional, philanthropic, and industry sources to create durable, long-term systems.
Redefining Success and Career Evaluation
A recurring concern was that success in the field remains narrowly defined and measured by institutional metrics like grants and publications, ignoring broader contributions to clinical care, policy, and innovation. Speakers called for expanded multidimensional promotion criteria, narrative curricula vitae, and distinct physician-scientist tracks that include reduced clinical expectations. However, any reforms must avoid creating new inequities—such as delaying advancement or overburdening faculty with documentation. Institutions should publish promotion and retention data to ensure transparency and accountability.
Strengthening Institutional and System-Level Commitment
Several panelists argued that hospitals and health systems prioritize clinical care and reimbursement, ignoring the value that research offers. Shifting this dynamic to treat research as a core element of their mission and creating models and mechanisms to support this element could be transformative. First steps may include integrating research metrics into health system performance and building learning health system models where research, care delivery, and data infrastructure are aligned.
Better defining the economic and societal value of the physician-scientist workforce could strengthen the case for sustained and value-based private investment. At the same time, “return on investment” must be broadly defined to capture long-term and public-good impacts—such as those in prevention, behavioral health, and social determinants of health—so that market-driven metrics do not inadvertently sideline essential but less commercially visible fields.
Elevating Advocacy, Communication, and Public Visibility
Participants emphasized that strengthening the physician-scientist workforce will require more deliberate and sustained advocacy. A central priority is securing multi-year federal funding commitments to provide greater stability and predictability across training and early-career stages, complemented by stronger state-level investment. At the same time, speakers underscored the importance of clearly articulating the value of physician-scientists to policy makers, institutional leaders, and the public. This includes equipping physician-scientists with communication and advocacy skills as part of medical education. Partnerships with patient groups and industry were also highlighted as important amplifiers, helping to humanize the workforce, demonstrate tangible impact, and reframe physician-scientists as directly serving patients and communities.
Building Early Engagement and Mentorship Networks
Participants across sessions emphasized early exposure and continuous mentorship as decisive factors in strengthening the physician-scientist pipeline. While some noted the value of outreach at the primary and secondary education level to broaden awareness and diversify the pipeline, undergraduate research may represent a more feasible and high-yield point for identifying and cultivating interested trainees. Suggested strategies included structured undergraduate research programs, bridge funding for gap years, cross-institutional mentoring networks, and formalized, monetized mentorship models that reward senior faculty for effective guidance. Building visible, connected communities was viewed as essential to countering isolation and ensuring that young scientists see a viable, well-supported path forward.
Conclusion
Dr. Dzau concluded that the physician-scientist is essential to patient care, discovery, and to the nation, but value must be articulated, visible, and measurable through stronger data, clearer communication, and a broader definition of success. Science today offers choices and frontiers that were unimaginable a generation ago, but questions and challenges remain regarding how to recruit more people to the medical sciences and how best to demonstrate to trainees and the public alike that this is a vibrant career path. Dr. Kwan also added that AJIA will work closely with partners, funders, and stakeholders over the coming months to guide action items to bring forth key solutions to current challenges facing the biomedical ecosystem and the workforce.
Sustaining this important workforce requires long-term commitment across the ecosystem—including stable funding, career-long support, and institutional investment that recognizes the vital role of physician-scientists. Models from Québec, Singapore, and leading US states demonstrate what is possible when compensation, protected time, and training are aligned. Additional individual suggestions put forth by workshop participants are outlined in Box 3. Beyond this discussion, more thought leadership and advocacy will be needed to align commitments and create multifaceted solutions to ensure the United States can continue to draw upon a strong and well-trained biomedical workforce.
Box 1 | Workshop Planning Committee Members
Jennifer M. Kwan, MD, PhD (co-chair), Yale University
Victor J. Dzau, MD (co-chair), National Academy of Medicine
Vivian G. Cheung, MD, Brown University
Ekta Dang, PhD, U First Capital Mukesh K. Jain, MD, Brown University
Brian K. Kobilka, MD, Stanford University
Brendan H. Lee, MD, PhD, Baylor College of Medicine
Robert J. Lefkowitz, MD, Duke University
Evan K. Noch, MD, PhD, University of Texas Southwestern Medical Center
SOURCE: Created by authors.
Box 2 | Workshop Speakers and Moderators
Jay Bhattacharya, MD, PhD, National Institutes of Health
Robert M. Califf, MD, Duke University
Vivian G. Cheung, MD, Brown University
Linda L. Demer, MD, PhD, University of California, Los Angeles
Victor J. Dzau, MD, National Academy of Medicine
Olivier Elemento, PhD, Weill Cornell Medicine
Ruben D. Flores-Saaib, PhD, Ligand Pharmaceuticals
Elena Fuentes-Afflick, MD, MPH, Association of American Medical Colleges
Sam Gill, MPhil, Doris Duke Foundation
David Ginsburg, MD, University of Michigan
Anna Greka, MD, PhD, Harvard University, Mass General Brigham, and Broad Institute of Massachusetts Institute of Technology and Harvard University
Carole Jabet, PhD, Fonds de Recherche du Québec
Mukesh K. Jain, MD, Brown University
Jennifer M. Kwan, MD, PhD, Yale University
Brendan H. Lee, MD, PhD, Baylor College of Medicine
Vivian S. Lee, MD, PhD, MBA, Harvard Business School
Michelle M. Le Beau, PhD, Cancer Prevention Research Initiative of Texas and University of Chicago
Robert J. Lefkowitz, MD, Duke University
Kenneth D. Mandl, MD, MPH, Boston Children’s Hospital and Harvard Medical School
Juanita Merchant, MD, PhD, University of Arizona
Louis J. Muglia, MD, PhD, Burroughs Wellcome Fund
Ivy Ng, MBBS, Singapore Health Services Pte. Ltd.
Evan K. Noch, MD, PhD, University of Texas Southwestern Medical Center
Kyu Y. Rhee, MD, PhD, Weill Cornell Medicine
John H. Sampson, MD, PhD, MSc, MBA, University of Colorado Anschutz School of Medicine
Yvette R. Seger, PhD, Federation of American Societies for Experimental Biology
Talia H. Swartz, MD, PhD, Icahn School of Medicine at Mount Sinai
Say Beng Tan, PhD, Singapore National Medical Research Council
Paul J. Utz, MD, Stanford University
Mary Woolley, Research!America
Joseph C. Wu, MD, PhD, Stanford University
Andrew R. Zinn, MD, PhD, University of Texas Southwestern Medical Center
SOURCE: Created by authors.
Box 3 | Suggested Ideas by Workshop Attendees
These suggestions represent a combination of ideas from pre-event and post-event surveys as well as in-person attendance. Because some are from survey responses, not all of these ideas are discussed in the preceding text.
Reimagine Education and Training Pathways
- Offer alternative, innovative medical school curricula with increased emphasis on basic science, and include opportunities for actual lab experience.
- Develop government-supported peacetime service programs for physicians in training that are highly incentivized and competitive and offer research training opportunities modeled after the Yellow Berets.
- Develop national high school research programs, promoting early talent development.
- Implement competency-based training models that replace rigid time-based requirements, enabling earlier transitions to independence without loss of rigor.
- Integrate research experiences continuously across medical, graduate, and residency training rather than as add-on phases, ensuring seamless progression.
- Expand debt-relief and salary-support mechanisms, such as loan-forgiveness programs, flexible NIH-cap policies, and bridge funding during training transitions, to sustain engagement.
- Encourage institutional accountability by reinvesting a portion of overhead or IP revenue into physician-scientist training endowments.
- Develop a program for MDs to earn a PhD during later residency or early faculty years to facilitate research continuity and smooth transition to independent research faculty positions in order to lower the average age at first R01.
Building Sustainable and Diversified Funding Ecosystems
- Use an amalgamated rate that provides competitive compensation and a salary that acknowledges research contributions.
- Use the number of postdocs moving on to independence as a metric of success for large grants.
- Expand institutional K awards by allowing universities to compete for K award slots so they have an existing position and can quickly hire an investigator to avoid delays.
- Directly obligate institutions to free clinician effort through shifted salary awards to ensure protected time is truly bought out and not theoretical.
- Provide institutional resources that reduce administrative burdens and develop mechanisms to support researchers across different career stages.
- Create protected time for research activities.
- Provide robust institutional support for salary and laboratory resources.
- Recruit fewer researchers but support them more comprehensively.
- Create gap year funding for MD and MD-PhD students.
- Strengthen sustainable federal funding for NIH, Agency for Healthcare Research and Quality, and Patient-Centered Outcomes Research Institute programs, with inflation-adjusted increases to preserve stability.
- Incorporate venture-philanthropy, public-private “moonshots,” and philanthropic endowments as complementary sources for long-term program stability.
- Reinvest a set portion of institutional royalties, licensing fees, and IP revenue directly into physician-scientist research and training funds.
- Pilot rapid-cycle or revolving-fund mechanisms to provide flexible bridge and seed funding for early-career investigators.
Redefining Success and Career Evaluation
- Create more flexible evaluation metrics that reduce administrative burden and recognize protected research time and collaborative contributions.
- Link research success to institutional value to persuade hospital leadership that supporting physician-scientists is financially and strategically beneficial.
- Develop more comprehensive metrics for evaluating scientific productivity.
- Expand definitions of success to include clinical innovation, policy influence, entrepreneurship, team leadership, and community impact.
- Recognize mentorship, teaching, and team-science leadership as integral to promotion and tenure decisions.
- Produce white papers that define institutional metrics for negotiation and progress tracking.
- Establish formal recognition systems and leaderboards to reward excellence in mentorship and collaborative science.
Strengthening Institutional and System-Level Commitment
- Include dedicated physician-scientist divisions, bridge funding, and administrative infrastructure to support career pathways.
- Increase the participation of physician-scientist role models in clinical teaching, rounding, and clinics (e.g., through co-attending model pairing with full-time clinicians). Vet them so only the most clinically adept are showcased and allow for integration of scientific insights.
- Encourage more risk-taking and novel science among junior investigators and directors.
- Create dedicated institutional research funds to guarantee internal stability when external grants lapse.
- Address structural disincentives such as NIH salary caps, rigid policies, and clinical-revenue pressures that discourage research engagement.
- Embed interdisciplinary hiring and cross-departmental mentorship to strengthen collaboration.
- Streamline administrative processes and reduce bureaucracy to protect time for discovery.
- Confront the cultural undervaluation of research and mentorship by aligning institutional incentives with scientific impact.
Enhance Advocacy and Public Communication
- Equip physician-scientists to communicate their work’s value to patients, policy makers, and the public; partner with patient advocacy groups; and incorporate advocacy training into curricula.
- Focus forward using new information channels and equip physician-scientists with skills to maintain relevance and public trust in communications.
- Invest in system-level solutions and better storytelling to highlight the importance of physician-scientist careers and the societal returns on investment.
- Integrate patient stories and tangible outcomes—such as new therapies or public health impacts—into institutional communications to demonstrate real-world benefit.
- Publicly promote physician-scientists’ dual role as healers and innovators driving national health and economic growth.
- Incorporate communication training programs and collaborations with popular media to normalize science storytelling (e.g., films, influencers, documentaries).
Building Early Engagement and Mentorship Networks
- Carefully select and support mentors.
- Build strong research communities within institutions.
- Create networking opportunities for early-career researchers.
- Build early exposure to research through pre-collegiate and undergraduate programs.
- Create cross boundary teams linking academia, tech, and industry to accelerate translation and reinvestment in careers.
- Establish formal mentorship networks and peer cohorts—including affinity groups for under-represented trainees—that promote belonging, recognition, and well-being, supported by institutional awards for mentorship excellence and integrated wellness and mental-health resources.
SOURCE: Created by authors.
References
AAMC (Association of American Medical Colleges). 2025. Medical School Graduation Questionnaire (GQ). Available at: https://www.aamc.org/data-reports/students-residents/report/graduation-questionnaire-gq (accessed November 7, 2025).
Browne, A. 2024. Prevalence and characteristics of physicians engaged in research in the US. JAMA Network Open 7(9):e2433140. https://doi.org/10.1001/jamanetworkopen.2024.33140.
Catenaccio, E., J. Rochlin, M. H. Akabas, L. F. Brass, and H. K. Simon. 2024. The financial impact of MD-PhD training compared with MD training for academic physicians. JCI Insight 9(24):e183476. https://doi.org/10.1172/jci.insight.183476.
Farhat, K., A. Obradovic, A. Siebert, H. N. Tun, E. K. Noch, and J. M. Kwan. 2025. Evaluating factors impacting early career physician-scientists’ decisions to continue research careers in the United States of America. BMC Medical Education 25:564. https://doi.org/10.1186/s12909-025-07144-4.
Jansen, C. S., A. Sugiura, L. Stalbow, C. Nguyen, J. P. Lever, A. Peiper, A. Plaza-Jennings, L. Varvel, M. A. Williams, A. Zarrinpar, and T. H. Swartz. 2023. Physician-scientist trainees with parenting responsibilities need financial and childcare support. Nature Medicine 29:2990-2992. https://doi.org/10.1038/s41591-023-02606-y.
Khot, S., B. S. Park, and W. T. Longstreth, Jr. 2011. The Vietnam War and medical research: Untold legacy of the US doctor draft and the NIH “Yellow Berets.” Academic Medicine 86(4):502-508. https://doi.org/10.1097/ACM.0b013e31820f1ed7.
Kwan, J. M., and C. P. Gross. 2023. Improving support for physician scientists—mind the (funding) gap. JAMA Network Open 6(9):e2332982. https://doi.org/10.1001/jamanetworkopen.2023.32982.
NIH (National Institutes of Health). 2014. Physician-Scientist Workforce Working Group Report. Available at: https://acd.od.nih.gov/documents/reports/PSW_Report_ACD_06042014.pdf (accessed November 7, 2025).
Packalen, M., and J. Bhattacharya. 2020. NIH funding and the pursuit of edge science. Proceedings of the National Academy of Sciences 117(22):12011-12016. https://doi.org/10.1073/pnas.1910160117.
Packalen, M., and J. Bhattacharya. 2019. Age and the trying out of new ideas. Journal of Human Capital 13(2):341-373. https://doi.org/10.1086/703160.
Pew Research Center. 2023. Americans’ trust in scientists, positive views of science continue to decline. Available at: https://www.pewresearch.org/wp-content/uploads/sites/20/2023/11/PS_2023.11.14_trust-in-scientists_REPORT.pdf (accessed November 5, 2025).
