Commission on Investment Imperatives for a Healthy Nation
Executive Summary
The activities of US health system organizations, including those operating in the health care sector, public health, and biomedical research, too often fail to align with the health goals and priorities of individuals and communities. In addition, these sectors do not effectively collaborate with each other or with other crucial sectors that influence health to strengthen alignment. Instead of being treated as active partners, individuals and communities are frequently viewed as passive recipients of health care, research, and public services, which neglects their expertise, experiences, and perspectives. Especially in the context of the revolutionary changes in personal health knowledge and control that artificial intelligence may enable, there is a clear need for new processes, structures, and cultures that support deliberative and democratic decision making. This moment presents an opportunity to better align all actions across the health sectors with the goals and priorities of the individuals and communities these sectors are meant to serve. To help inform a path forward, including the work of the Commission on Investment Imperatives for a Healthy Nation, the National Academy of Medicine (NAM) convened an expert working group to outline a shared vision and potential actions for ensuring that the goals and priorities of individuals and communities are the orienting reference points for every health sector decision and action. This critical reorientation has the potential to build trust throughout the health system.
To start, this discussion paper presents background on recent trends and the current state of individual and community engagement across US health sectors (health care, public health, and biomedical research), including engagement shortfalls and driving factors hindering progress. These interconnected drivers (see Figure 1) include the need for inclusive structures and metrics to promote meaningful engagement; a holistic definition of health that goes beyond physical disease; multidirectional trust between health sector organizations, individuals, and communities; a financial ecosystem that aligns with individual and community health goals; a well-equipped and accountable health sector workforce; and the effective use of data and evidence to inform decision making. To underscore the imperative for action, the authors share the societal costs of maintaining existing practices, including significant impacts for individual and community health and well-being, professional domains, and the broader economy.
In accordance with the working group’s charge, the authors outlined a menu of solutions and levers to guide health sectors toward authentic engagement of and accountability to individual and community health goals and priorities. The solutions described, along with the possible gains and outcomes at the individual, community, and societal levels from enacting them, include establishing a holistic perspective of health, promoting collaboration and shared decision making, investing in individual- and community driven research, and investing in a person- and community-centered workforce. These solutions are grounded in the need to adopt radical empathy through bidirectional learning and listening. Such a foundation will help promote deep understanding of the complex interplay between individual and community-level factors, cultivating a culture of accountability rooted in caring, mutual relationships while honoring any necessary procedures.
Potential stakeholders who could advance these solutions by activating these levers include the US health sectors mentioned; corresponding governing bodies; philanthropic groups that fund these sectors; and governmental, institutional, and community leaders and advocates in sectors critical to establishing vital conditions that enable individuals and communities to live healthfully. Important to consider when identifying the best solutions and levers to prioritize, adapt, and apply are the national, state, and local contexts, which will continue to evolve and shape health and well-being over time. To conclude, the authors emphasize that building the momentum for meaningful change will likely require sharing accountability structures, promoting collective action, and advancing strategic approaches to capability development. These momentum builders include a “bottom-up” approach, where local actors work together to develop solutions tailored to their unique contexts. In that regard, each individual and community member would bring their experiences, expertise, and other assets that can be leveraged in these relationships and activities to drive real-world change over time. Concurrently, momentum can also be accelerated through “top-down” policies and structural changes that enable these shifts and provide needed funding.
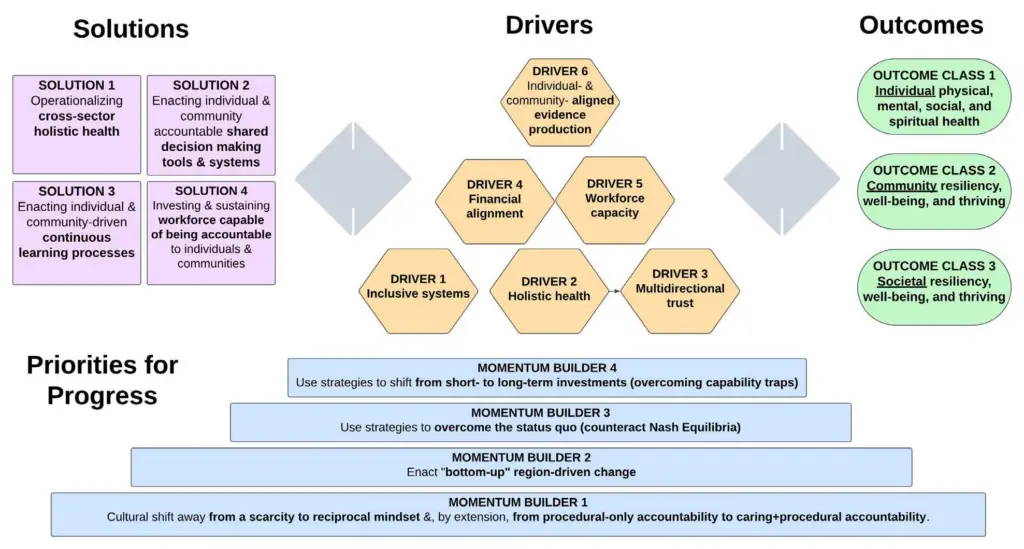
FIGURE 1 | Summary of Solutions Mediated by Targeted Drivers to Outcomes with Key Momentum-Building Strategies to Marshal the Momentum for Change
SOURCE: Created by authors.
Introduction
Radical empathy, on the other hand, means putting in the work to educate yourself and to listen with a humble heart to understand another’s experience from their perspective, not as we imagine we would feel. Radical empathy is not about you and what you think you would do in a situation you have never been in and perhaps never will. It is the kindred connection from a place of deep knowing that opens your spirit to the pain of another as they perceive it. (Wilkerson, 2020, 386)
This call for radical empathy speaks to a fundamental reorientation needed across health sectors—one that recognizes that people are complex, layered beings not reducible to only patient identities (Brown, 2017). The core challenge is to identify how to invest in and create relational systems and spaces where a wide range of expertise and experience at the professional, individual, and community levels are all recognized as essential and complementary forms of knowledge and skill. Then individuals, communities, and health sectors can cultivate mutual understanding and inform actions to improve health and well-being across the nation.
A step forward in recognizing the importance of diverse perspectives came with the publication of an important 2012 article in the New England Journal of Medicine by Michael Barry and Susan Edgman-Levitan. This article laid out foundational principles for patient-centered care, calling on physicians “to relinquish their role as the single, paternalistic authority and train to become more effective coaches or partners—learning, in other words, how to ask, ‘What matters to you?’ as well as ‘What is the matter?’” (Barry and Edgman-Levitan, 2012, 781). Rather than existing as paternalistic authorities, health sectors have essential roles to play as partners in advancing individual and community health goals and priorities. More recently, person-centered care has been recognized as crucial for improving care delivery and health outcomes (Watson et al., 2024). “Person-centered care means that individuals’ values and preferences are elicited and once expressed, guide all aspects of their health care, supporting their realistic health and life goals. Person-centered care is achieved through a dynamic relationship among individuals, including those who are important to them, and all relevant providers. This collaboration informs decision making to the extent that the individual desires” (American Geriatrics Society Expert Panel on Person-Centered Care, 2016, 16). The body of evidence on the benefits of person-centered care has continued to grow, as well as the identification of approaches and models to provide person centered care planning (AHRQ, n.d.).
Over the last several years, there has also been a growing recognition of the role of the communities with which individuals identify and the importance of meaningfully engaging these communities to achieve their desired goals and priorities, as well as advance health equity through transformed systems for health (Organizing Committee, 2022). Critically, this recognition extends beyond viewing communities as care recipients to honoring them as powerful actors capable of defining priorities, mobilizing resources, and driving change. While this discussion paper focuses on decisions and actions at the system level, the authors emphasize that both communities and individuals possess “civic muscle”—the capacity to shape their lives by organizing, advocating, and holding systems accountable (Milstein et al., 2023). Creating conditions where all people can thrive requires rejecting false binaries. This is neither solely a systems problem requiring only policy reform, nor solely an individual problem requiring only personal resilience. Rather, it demands a both-and orientation: both honoring and strengthening individual and community agency and capacities and simultaneously transforming the systems and structures that enable or constrain that agency.
Health sector misalignment with individual and community goals and priorities remains a persistent issue. In the health care system, misalignment arises from an overemphasis on treating symptoms, acute conditions, and other challenges, rather than addressing root causes and investing in preventive services and person centered care. Reimbursement models often prioritize volume over value and outcomes (i.e., wellness), reinforcing the imbalance. Within the health science enterprise, misalignment often appears when research priorities are developed and dictated by the research community, with minimal recognition of the knowledge and limited accountability to individuals and communities impacted. Within public health systems, misalignment occurs through a lack of effective democratic structures that enable the prioritization of public funds to invest in and maintain the infrastructure needed to enable communities to withstand and recover from sudden, disruptive events. This is true not only for foundational public health services, such as the coordination of vaccine services and health promotion campaigns, but also in robust collaboration across critical sectors that influence health, such as food, housing, transportation, public safety, education, economic development, and environmental sustainability. Traditional health sectors do not effectively collaborate with each other or with other crucial sectors that influence health, and the lack of coordination hinders the creation of essential vital conditions that enable everyone, in every community, to have the opportunity not just to survive but thrive.
To advance a shared vision in which individual and community goals and priorities serve as the orienting reference points for every health sector action and decision, the authors propose a menu of solutions and levers for fostering authentic engagement and accountability. These approaches are grounded in radical empathy and supported through bidirectional learning and listening between health sectors and the people they serve. These practices promote understanding experiences from the perspective of others, rather than relying on assumptions, while also enabling individuals and communities to understand any constraints and challenges health sectors encounter. The combination of these practices, along with robust accountability and engagement structures, can help health sectors establish a guiding framework for decision making that aligns the expertise of health sectors, individuals, and communities.
Defining Key Terms, Frameworks, and Models
To provide a clear foundation for the subsequent discussion, it is essential to define key terms (see Box 1), frameworks, and models used throughout this discussion paper. The authors recognize that these concepts can be subject to multiple interpretations, and the definitions presented here are intended to facilitate a shared understanding and inform the development of a vision for addressing the pressing challenges of alignment and accountability in the US health and well-being landscape.
BOX 1 | Key Terms
Individuals: In the context of health and health care, the term individuals refers to anyone—including patients, families, caregivers, and community residents—interacting with or connected to those interacting with the health sectors noted below.
Community: This discussion paper uses the definition of community provided in the second edition of the Principles of Community Engagement by the Centers for Disease Control and Prevention (CDC): “groups of people affiliated by geographic proximity, special interest, or similar situations” [a]. The latest edition released in 2025 adds to this definition, describing the transitory nature of communities, and that an individual’s affiliation with and/or identification with a community can be complex and dynamic [b].
Health: “A state of complete physical, mental, and social well-being and not merely the absence of disease or infirmity” [c].
Health sectors: In this discussion paper, the term health sectors consists of health care systems, the health science enterprise, and public health systems, each of which are explored in more detail below. It is critical to emphasize that health does not occur solely within the siloes of these traditional health sectors. Many systems and contextual factors across diverse settings heavily influence health status (social determinants of health or SDOH), and coordination among these systems and factors is critical. Additionally, some organizations may apply to more than one of the three sectors.
- Health care system: The health care system can be defined as a collection of interconnected organizations that support the administration, diagnosis, treatment, and prevention of physical, behavioral, and mental diseases or illnesses through various levels of medical care and coordination. This system includes clinicians and other care providers, insurance plans, self-insured employers, labor unions, administrative and regulatory structures, health technology, pharmaceutical industry, biotechnology, and health financing that facilitates the management of disease [d].
- Health science enterprise: The health science enterprise includes academic, nonprofit, independent, industry researchers, organizations, institutions, and federal agencies (including the National Institutes of Health, Agency for Healthcare Research and Quality, Centers for Disease Control and Prevention, and Patient-Centered Outcomes Research Institute) seeking to produce and use knowledge to enhance health and well-being. Their activities are often guided and supported by federal agencies, philanthropic and funding organizations, and other relevant parties or sectors.
- Public health system: For the public health system, this discussion paper uses the definition provided by the National Association of County and City Health Officials: “Public health systems are commonly defined as ‘all public, private, and voluntary entities that contribute to the delivery of essential public health services within a jurisdiction ’” [e]. Public health systems can also be described as a network of entities with different roles, relationships, and interactions that contribute to the public’s health [e]. For example, state and local governmental public health departments are crucial stakeholders but do not provide the full spectrum of essential public health services alone [e].
Health equity: This piece also uses a Robert Wood Johnson Foundation definition of health equity: “that everyone has a fair and just opportunity to be as healthy as possible” [f].
SOURCES: [a] CDC (Centers for Disease Control and Prevention). 2011. Principles of community engagement. 2nd ed. Washington, DC: National Institutes of Health. Available at: https://stacks. cdc.gov/view/cdc/11699 (accessed May 23, 2025). [b] CDC. 2024a. Principles of community engagement. 3rd ed. Washington, DC: CDC and Agency for Toxic Substances and Disease Registry. Available at: https://cohnlabs.org/principles-of-community-engagement (accessed May 27, 2025).[c] WHO (World Health Organization). n.d. Constitution. Available at: https://www.who.int/about/ governance/constitution (accessed May 23, 2025). [d] American Hospital Association. 2017. Federal Agencies with Regulatory or Oversight Authority Impacting Hospitals. Available at: https:// www.aha.org/system/files/2018-01/info-regulatory-burden-federal-agencies.pdf (accessed May 23, 2025). [e] National Association of County and City Health Officials. n.d. The Public Health System. Available at: https://www.naccho.org/uploads/downloadable-resources/Programs/ Public-Health-Infrastructure/Defining-Terms-The-Public-Health-System.pdf (accessed May 23, 2025). [f] Robert Wood Johnson Foundation. 2017. What is health equity? Available at: https:// www.rwjf.org/en/insights/our-research/2017/05/what-is-health-equity-.html (accessed March 24, 2026).
Vital Conditions for Health and Well-Being (the Vital Conditions Framework)
Regarding key frameworks, the Vital Conditions for Health and Well-Being Framework (see Figure 2), referred to as the Vital Conditions Framework moving forward, articulates upstream factors foundational for people to reach their full potential (HHS, 2022). It presents an actionable, asset-based approach to improving the social determinants of health (SDOH) and addressing inequities and disparities (HHS, 2022; Milstein et al., 2023). At the center of this approach are belonging and civic muscle. Belonging refers to the cultivation of strong social connections, fulfilling relation-ships, and a sense of being valued and supported within a community (HHS, 2022). Individuals do not exist in isolation—they are influenced by and help shape the communities with which they identify and in which they live. Civic muscle refers to the cultivation of processes, structures, systems, and cultures that nurture individuals’ and communities’ capacities in engaging in civic life, including voting, decision making, and working together to collec-tively address challenges and opportunities (HHS, 2022). These two elements emphasize the critical role of civic engagement in building community capacity, as well as the imperative nature of local, self-driven, and tailored solutions in meeting needs and fostering an equitable future (HHS, 2022).

FIGURE 2 | Vital Conditions for Health and Well-Being
SOURCE: The Rippel Foundation. n.d. Vital Conditions for Health and Well-Being. Available at: https://rippel.org/vital-conditions (accessed April 11, 2025).
Learning Health System’s Shared Commitments Trust Framework
The second underlying framework in this discussion paper, the Learning Health System’s Shared Commitments Trust Framework, has been stewarded by the NAM since 2006 when the Learning Health System (LHS) was conceived and embedded in the charter of what is now the NAM Leadership Consortium, composed of stakeholder sector leaders from across health and health care. LHS is defined as “one in which science, informatics, incentives, and culture are aligned for continuous improvement, innovation, and equity—with best practices and discovery seamlessly embedded in the delivery process, individuals and families as active participants in all elements, and new knowledge generated as an integral by-product of the delivery experience” (McGinnis et al., 2024). Table 1 presents the commitments and expectations embedded in this framework to provide common ground aims for every organization engaged in the advancement of health.
TABLE 1 | Shared Commitments: A Trust Framework for Continuously Learning Health System
| Engaged | Gives primacy to understanding, caring, and acting on people’s goals. |
| Safe | Deploys verified protocols to safeguard against risk from unintended harm. |
| Effective | Applies continuously updated evidence to target goal achievement. |
| Efficient | Delivers optimal outcomes and affordability for accessible resources. |
| Fair | Advances parity in individual opportunity to reach full health potential. |
| Accessible | Provides timely, convenient, interoperable, and affordable services. |
| Accountable | Identifies clear responsibilities, measures that matter, and reliable feedback. |
| Transparent | Displays full clarity and sharing in activities, processes, results, and reports. |
| Secure | Embeds safeguards in access, sharing, and use of data and digital/AI tools. |
| Adaptive | Centers continuous learning and improvement in organizational practices. |
SOURCE: NAM. n.d. Learning health system shared commitments. Available at: https://nam.edu/our-work/programs/leadership-consortium/learning-health-system/ (accessed January 14, 2026).
Presenting a Shared Vision
Individual and community health goals and priorities, as defined by individuals and communities, should serve as the primary reference point for all decisions and actions across health sectors. As noted in the description of the health sectors represented in this discussion paper, the achievement of these goals is influenced by an interplay of many factors, including factors within and outside these traditional sectors, that add multiple layers of complexity to how people interact with and experience health and well-being. For individuals, health-related social needs and sociodemographic characteristics, including cultural background and socioeconomic status, are crucial determinants of health behaviors and outcomes. For instance, cultural beliefs and experiences of bias and harm, including mistrust of health care providers and systems, can shape perceptions of the health sectors, ultimately impacting trust and willingness to seek care. Similarly, socioeconomic status affects access to essential conditions, such as nutritious food, safe housing, and quality health care, which are vital for enabling individual and community health and well-being.
On a broader scale, community-level factors, including demographic characteristics, environmental factors, social policies, and systemic favoritism, significantly influence health outcomes. Similar to the individual level, sociodemographic characteristics can also determine care access, availability, and quality, as well as the range of public services community members can receive. Environmental factors, like air and water quality, and access to green spaces, contribute to community well-being. Moreover, systemic issues, such as policies that favor one group over another, can create barriers that further hinder communities from receiving the investment, infrastructure, and, ultimately, public services needed to achieve optimal health and well-being and adapt to new circumstances when needed. Understanding the interplay between these factors is crucial for guiding within and cross-sector decision making that is effective, efficient, and fair. For example, a person’s efforts to maintain a healthy lifestyle can be undermined by living in a community with limited access to basic needs like healthy food and safe spaces for physical activity. Conversely, communities with robust social networks and supportive environments can enhance individual health efforts, leading to better overall outcomes. However, there is a lack of concrete requirements for health sectors to engage individuals and com-munities in decision making, making it challenging to establish accountability systems and structures that are aligned to individual and community goals and priorities. For example, there are neither a clear governing body nor clear targets or mandates set by many payers that require health care organizations and workers (including nurses, medical technicians, physicians, and C-Suite executives) to meaningfully listen to, engage with, and align actions in a person-centered way. With this, there is a lack of structures to monitor and improve the quality of knowledge and guidance on clinical and medical decisions or the degree to which alternative options are robustly explored. To illustrate, although patient portals have increased access to medical records, many patients still lack the back-ground or guidance needed to understand how to access and interpret this information, preventing them from making informed decisions about their health and care. Furthermore, communities lack mechanisms to hold health care organizations accountable for their community engagement and prevent potential harm to the community.
Embracing the Vital Conditions Framework and the LHS Shared Commitments Trust Framework, there are significant opportunities to strengthen the engagement of individuals and communities in decision making within and across health sectors. Health sectors that hold individual and community health goals and priorities as the orienting reference point in their decisions and actions and are authentically accountable to them would help drive and achieve optimal health and well-being across physical, mental, social, and spiritual domains. For each focal sector, this could translate to the following, with more details on overarching solutions, levers, and specific examples presented later in this discussion paper. While each sector has its own outlined vision and actions below, several elements can apply across the sectors.
A health care system that delivers effective, integrated, coordinated, sustainable, and person-centered primary, secondary, tertiary, and quaternary care for physical, behavioral, and mental diseases could be accomplished by the following actions:
- Develop and sustain authentic relationships built on multidirectional trust and trustworthiness that allow for continuous learning and empowerment between health care organi-zations, individuals, and communities. For example, this could occur through democratic and deliberative forums that provide individuals and communities with opportunities to contribute to and influence health care system-level decisions. These system-level changes could then be monitored by how well health care environments enable clinicians and other providers to build authentic relationships and align their decisions and actions with patient health goals and priorities, as assessed by patients, communities, and those who provide care.
- Equip future health and health-related workforce with the appropriate skills and a safe environment to understand and integrate individual and community health goals and priorities into their practices and engagement, fostering a holistic approach that ensures access to comprehensive services across other sectors.
- Partner with and support other sectors (such as transportation, urban developers, education, and agriculture) positioned to invest in vital conditions to advance optimal health. These changes could be monitored and managed through reimagined public health system and health science enterprise actions mentioned below, with both sectors incorporating clear metrics and monitoring systems of resource and information flow across sectors.
A shift to a public health system that cultivates belonging and civic muscle could be supported through the following actions:
- Support “local-first” federated public health systems (including at the city, county, state, and national levels) that create collaborative spaces, enact local and regional democratic-led processes, and promote shared decision making efforts within the health sectors and across all sectors that support the vital conditions of health and well-being. With these actions, public health system monitoring would focus on the degree to which these systems can effectively support belonging and civic muscle and foster mutual accountability across public service sectors to achieve optimal community health.
- Sustain infrastructure across public, private, and voluntary entities to create a central coordinating mechanism that strengthens belonging, civic muscle, and community
A health science enterprise to expand their role beyond general knowledge production, application, and dissemination, including individuals and com-munities in research codesign and the cocreation of evidence, would consider the following activities as essential to their role:
- Advance an actionable research agenda explicitly driven by and accountable to individual and community goals and priorities. These changes could occur and be continuously monitored via tracking funding announcements and corresponding review panel calls across health science enterprise funders to support a critical mass of funding available for research explicitly aligned with individual and community goals and priorities. This could also be monitored by the federated sharing of individual and community goals and priorities, which would be managed, curated, and then shared via a LHS infrastructure that enables effective communications within and across health sectors, as well as broader sectors that impact health (Bierman and Mistry, 2023).
- Conduct research to improve processesvneeded to foster meaningful relationships and authentic accountability between individuals, communities, and health science enterprise institutions. This activity could be monitored and seek to be in service to the public health system’s efforts to support civic belonging and civic muscle, focusing explicitly on the health and vitality of relationships between research institutions and communities and the regions with which communities identify. This could also be enacted within the LHS infrastructure described earlier.
Status and Trends on Individual and Community Engagement
As mentioned in the introduction, there has been a growing recognition of the importance of engaging with individuals and communities across health sectors to achieve optimal health and well-being, promoting health for everyone, in every community. This approach prioritizes learning from and understanding the health and life priorities of individuals and communities. A fundamental principle of health advocacy, first articulated by the disability rights community, is “Nothing about me without me” (Charlton, 1998, 3). This principle can only be realized by understanding what matters most to individuals and communities.
Historically, health sectors have employed a top-down approach, relying on traditional experts, such as academics, physicians, and policy makers, to determine and implement health priorities without adequate input from those directly impacted or accountability to those being served. However, building on several decades of progress, a significant shift is underway, driven by the recognition that individuals and communities are best positioned to understand their unique contexts, cultures, and circumstances. As a result, there is a growing demand for more inclusive and participatory models of health governance, where health is not only available but also accessible, culturally appropriate, and driven by the voices, values, and priorities of those directly impacted (Teisberg et al., 2009).
Engagement Across the Health Sectors
Health Care Systems
Health care systems have increased efforts to provide person-centered, culturally tailored care, fostering trust and encouraging greater engagement between health care systems, individuals, and communities. In addition, emphasis on the impact of social contexts (SDOH) and unique health-related social needs (HRSN) have stimulated health care systems to address health more holistically. With a growing recognition of the importance of addressing HRSN, the Accountable Health Communities Model, an initiative led by the Centers for Medicare and Medicaid Services (CMS) from 2017 to 2022, addressed HRSN through enhanced clinical-community linkages to improve health outcomes and reduce costs (CMS, n.d.; Health Affairs Forefront, 2023). The model screened Medicare and Medicaid beneficiaries for five HRSNs and offered eligible beneficiaries assistance in accessing community-based social services, with a designated cohort receiving navigation support (RTI International, 2024). Health navigators built trust and completed patient-centered action plans to understand patients’ lives and help them achieve their health goals. Researchers found that Medicaid and fee-for-service Medicare beneficiaries receiving social services through health navigators had lower total health care costs than those who did not receive navigation services (RTI International, 2024). Over the past decade, the percentage of US hospitals screening for HRSN grew substantially, with over 60 percent of hospitals screening in 2019, up from just 25 percent in 2015 (Ashe et al., 2023).
The growing role of technology and digital platforms has further expanded engagement in health decision making by enabling communication between care recipients and historically recognized health authorities (such as clinicians) outside of physical medical visits (Yeung et al., 2023). Digital health tools, such as social media, mobile health apps, and online forums, have increasingly allowed individuals and communities to voice their concerns and share information (Chen and Wang, 2021). For example, the adoption of patient portals increased 24 percent between 2020 and 2022, with 57 percent of individuals in the United States accessing their patient portals or online medical records at the time (ASTP, 2023). Additionally, wearables and sensors that track health, from chronic disease management to wellness, reflect an upward trend in seven years from 9 percent to 21 percent (Vogels, 2020). Access to more information and data may empower patients to engage in more meaningful discussions, fostering a collaborative approach with health care providers to help facilitate greater involvement in their health and wellness.
For younger demographics, individuals in under-resourced communities (such as older adults, rural residents, and more), and those previously left behind by traditional and ineffective engagement strategies, this digital shift has proven especially transformative for real-time and inclusive care (Abernethy et al., 2022). However, broadband access continues to be irregular across these communities and across certain demographics, the integration of digital health technologies into clinical practices and tools is still ongoing, and patient- and community-reported data points are often underused in adjusting health care treatments (Zhang and Saltman, 2022; Cain et al., 2022). It is critical not to overlook these challenges in enabling access to digital technologies and e-health services, especially with the acceleration of artificial intelligence.
Health Science Enterprise
Across the health science enterprise, there has been increased attention to community-based participatory research, patient-centered outcome research, and codesign methods. These methods engage individuals and communities throughout the research and decision making processes so that health interventions are designed, developed, tested, deployed, and continually monitored and adapted to produce culturally sensitive, contextualized interventions that fit individual and community circumstances and needs. Additionally, there have been increasing investments in developing a new generation of researchers that reflect underrepresented and under-resourced communities. Overall, these trends reflect a broader recognition of the importance of equity and social justice in health, acknowledging that individuals and communities in marginalized conditions must have a voice in shaping the policies and programs that affect them.
Public Health Systems
Responsibility for engaging individuals and communities in decision making processes lies partially with public health systems and their partners as well. This work has been prioritized due in part to requirements for formal Community Health Needs Assessments (CHNAs), which the Internal Revenue Service (IRS) also requires for nonprofit hospitals. These CHNAs encompass the assessment and planning processes that nonprofit hospitals carry out on a three-year cycle to maintain their nonprofit status as mandated by the Internal Revenue Service (IRS, 2024). Additionally, Community Health Assessments (CHAs) are carried out by local health departments to maintain their voluntary accreditation by the Public Health Accreditation Board (PHAB, 2016). Both entities create and conduct Community Health Improvement Plans (CHIPs) based on CHNA/CHA findings.
However, these responsibilities do not preclude diverse collaboration across stakeholders. For example, because CHAs are not required by law, only for accreditation, it can be difficult for public health departments to obtain the necessary resources to support effective community engagement specific to a CHA process. Nonprofit hospitals are required by law, but they still also face challenges in the time-intensive process of conducting CHNAs and developing implementation strategies. The translation of CHNA and CHA priorities into actionable measures targeting SDOH demands substantial resources—people, processes, time, and energy. More recently, public health departments and hospitals have been collaborating to complete these processes to improve community health (Cramer et al., 2021).
Engagement Shortfalls and Salient Contributors to the Problem
Individual and community engagement at the national, state, and local levels vary significantly across health sectors, leading to differing degrees of meaningful impact and, alternatively, health shortfalls. Lack of meaningful engagement between individuals, communities, and health sectors can lead to miscommunication, distrust, ineffective interventions, the reactive or inefficient use of health care services and resources, overuse of low-value health care, barriers to treatment adherence, loss of community resilience, and worsening health inequities. Actively engaging individuals and communities as leaders and partners in decision making processes through transparency, shared accountability, and trust-building can result in more inclusive and effective health sectors that adequately meet the diverse needs of varying populations. Unfortunately, US health sectors have struggled to align, prioritize, fairly conduct, and invest appropriately in authentic engagement for improved health outcomes due to many driving factors and with systemic barriers at the core of those factors.
Systemic Barriers
Groups who are socioeconomically disadvantaged or living in marginalized conditions persistently face systemic barriers to engagement and disenfranchisement rooted in structural discrimination, access to information, and environmental barriers. The procedural focus of health sector policies and interventions often excludes key engagement from community leaders and advocates who may be able to shed critical viewpoints and perspectives to improve communication, improve interventions, and maximize resources. For example, meeting formalities, such as the use of jargon or complex language; meeting formats that limit interaction or discussion; insufficient meeting notice and duration; and inaccessible meeting facilities, equipment, and other accommodations for people with disabilities and those who require language interpretation, pose barriers to effective engagement. Failure to value individual and community voices and knowledge and prioritize engagement has resulted in many people in the United States being excluded from participating in policy change efforts aimed at addressing health inequities and social conditions that contribute to them (ChangeLab Solutions, 2019). Exclusion from engagement can lead to a sense of powerlessness; perceived disconnection and social isolation; and distrust of institutions, organizations, and systems. This can foster apathy and opposition among community members, which highlights the tension between government public health measures and individual civil liberties.
Structural racism is a form of racism that is “pervasively and deeply embedded in systems, laws, written or unwritten policies, and entrenched practices and beliefs that produce, condone, and perpetuate widespread unfair treatment and oppression of people of color” (Braveman et al., 2022). Structural racism fosters hostile environments that discourage participation among lesbian, gay, bisexual, transgender, queer, or questioning groups/populations; immigrants; people with disabilities; and other historically marginalized groups (Snyder et al., 2018). The underrepresentation of disenfranchised groups in decision making roles within government and organizational structures, where institutional leaders and elected officials do not reflect the values and the demographic makeup of populations served, can lead to decreased knowledge of and responsiveness to their needs, exacerbating feelings of disenfranchisement. Historically marginalized community members’ contributions may be undervalued or ignored, reinforcing the notion that they are not entitled to engage in decision making processes. The mental health toll (increased anxiety and depression) of racism can diminish individuals’ capacity to engage with their community. Such experiences are further heightened by the intersection of race and other social identities. Undocumented immigrants face additional challenges that prevent them from fully participating in community health initiatives, including language barriers, fear of deportation, and lack of access to insurance and health services.
Socioeconomic Inequities
Socioeconomic inequities represent the broader consequences that result from systemic barriers and further limit opportunities for individual and community engagement in health decisions. Persons from lower-income backgrounds often lack the resources (such as paid time off, transportation, child care, elder care) necessary to participate fully in government hearings, community health planning meetings, or advisory groups such as patient and family advisory councils. Many organizations within health sectors have missions and values that state integrity, transparency, and collaboration; however, many fail to include those who have experienced trauma, biases, and harm or had limited access to education and employment when partnering and codesigning solutions, which is a common thread throughout all engagement shortfalls mentioned.
Limited Definition of Health
The core prioritization challenge is reinforced by the continued limited definition and operationalization of health. While there has long been a recognition of the broad nature of health that goes beyond the absence of physical and mental disease, the health sectors continue to default back to a narrower definition and approach to health that primarily focuses on disease and providing “sick care.” There is an overemphasis on and substantial capacity allocated to measuring and influencing diagnosis, treatment, and prevention of physical and mental diseases. This directly contrasts with the long-recognized holistic definition of health used by the World Health Organization (WHO) and the broader understanding of the drivers of health equity.
Lack of Multidirectional Trust
A lack of trustworthiness and trust are significant obstacles limiting authentic individual and community engagement. Trust is essential for delivering quality and respectful care, yet it is in decreasing supply, particularly within historically marginalized communities. Individuals and communities often distrust health sector actors because of experiences of racism, provider bias, health sectors’ predatory business practices, growing exposure to misinformation or disinformation, and other experiences of systemic oppression.
Notably, there is a common misconception regarding individuals who are described as “not trusting the health care system,” especially when this concept is often discussed in the context of racial groups. Mistrust and distrust largely stemming from historical and present injustices, such as unethical government-led medical experiments (e.g., the US Public Health Service Study of Untreated Syphilis in the Negro Male at Tuskegee and Macon County, Alabama 1932-1972) and mistreatment of Black, Indigenous, and other persons of color (e.g., inadequate distribution of quality, affordable health care providers and vital social resources) have left lasting scars (Sterling, 2011). Additionally, numerous studies note that health care system providers do not trust or listen to their patients of color, often resulting in stark disparities in care (Grob et al., 2019). This bidirectional lack of trust stems also from the lack of representation that community members see in their health care providers and the transactional nature of health care delivery necessitated by the financial system underpinning it.
Misaligned Financial Incentives and Financial Structures
Perhaps a fundamental core problem is the financial ecosystem within which care is paid for and health and social care providers operate. Cost and insurance barriers dictate what providers, procedures, medications, and equipment a patient can access. Additionally, complex incentives confront providers with trade-offs between their own self-interest and patient interests. Providers on the frontlines of health care delivery, especially those serving populations with significant health disparities and inequities (e.g., Medicaid and Medicare beneficiaries, uninsured and undocumented individuals) can be governed by the following factors:
- Fee-for-service structures, which incentivize providing more care, regardless of quality, and do not consider issues of access;
- Quality measures rooted in safety and clinical guidance that incentivize transactional approaches to care, even for measures such as patient satisfaction; and/or
- Short-term cost reduction through value-based arrangements designed and overseen by payers incentivized to ration and gatekeep care rather than to optimize care delivery in alignment with patient goals and priorities.
While patient experience is a frequently collected metric that can impact reimbursement, it rarely relates back to patient or community health goals (Berkowitz, 2016). There is an increasing movement by payers to develop alternative payment models and associated measures and metrics that better reflect patient goals and priorities (Adler-Milstein et al., 2025). However, these models, and the data to support them, can be complicated to design and tend to require substantial investments in time and infrastructure to implement (US Government Accountability Office, 2021).
Many people who enter the health care field are intrinsically motivated to build healing relation-ships with patients, but the financial structure of the health care system often limits the time available for meaningful engagement. Because payment is linked to various measures, providers may find their time occupied by closing gaps in care, improving documentation to optimize billing, and submitting prior authorizations to insurance companies, instead of interacting with patients and their goals. Examples of engagement anchored by transactional structures can look like community advisory councils with insufficient investment in participating community members, or sponsorship of community events that raise awareness of services but does not allocate time or resources to create sustained relationships or continuous feedback loops with community members.
Workforce Issues
As mentioned, there has been a shift away from traditional models of care toward teaching care that embraces the authentic engagement of individuals and communities. However, health sectors still lack accountability tools to determine whether those models and specific strategies have achieved individual and community health goals and priorities.
At the individual provider level, effective patient engagement in curricula and professional training still vary in amount and depth, often assuming a “one and done” approach. While there has been more investment in training on helpful topics such as motivational interviewing, trauma-informed care, implicit bias, narrative medicine, and other patient-centered frameworks, they are rarely prioritized over training on risk reduction and revenue-generating activities, such as safety, quality, compliance, and operations (Glasberg, 2023). These misplaced priorities are often driven by barriers created from the financial incentives and structures mentioned earlier. Board and senior leadership accountability may not be directly tied to the success of reaching these goals and priorities. As a result, teams responsible for engagement may also be under-resourced or siloed from an organization’s financial and organizational strategy.
Rising workforce shortages across medical disciplines are increasingly hindering access to care and services, and are particularly severe in primary and geriatric care (Jabbarpour et al., 2025; Collins and Kaine, 2025). Compounding this issue, the current health sector workforce does not proportionately reflect the racial, ethnic, and socioeconomic backgrounds of the individuals and communities they are meant to serve. While the community health worker movement has enabled the integration of cultural congruence onto care teams, these positions are poorly paid and often lack structured professional development pathways that allow their perspectives to reach decision making positions. As a result, valuable insights and the development of meaningful engagement tactics that could occur at the organizational level rarely receive the investment and attention needed.
Creation and Application of Data and Evidence
Health disparities are propagated, in part, due to an overreliance on traditional research methods that, when used alone, do not produce all the evidence needed to support effective decision making. As a result of the COVID-19 pandemic, there has been a resurgence in the need for and understanding of why better data collection, analysis, and reporting across the health sectors are essential to improving individual and community health. Despite the vast amount of data generated by health sectors from electronic health records and clinical and public health research, these sectors continue to struggle with collecting, synthesizing, and leveraging data that accurately represent and benefit individuals and communities, especially historically marginalized and underrepresented populations. In addition, certain data have increasingly been removed from the public domain, or the collection of specific data sets has been discontinued.
The availability of accurate, user-friendly sociodemographic data is essential to addressing persistent health inequities and disparities. Access to this data is also helpful to individuals, communities, and researchers to support planning, decision making, and resource allocation to improve overall health. For example, efforts to disaggregate ethnic data and collect sexual orientation and gender identity data can help unmask disparities and identify specific health concerns within these groups. Inaccurate or incomplete data collection can lead to the misinterpretation of health trends and result in limited research aimed at improving the health and well-being of individuals in these subgroups. Additionally, the ways in which data are protected, stored, shared, and regulated are also important considerations. People have privacy and security concerns about how data can be used against them, such as the potential for care to be denied or for biases and stigmas to affect the quality of care they receive.
Beacons of Hope
Despite these enumerated opportunities and challenges, in recent years, important advances have been made in the appreciation, application, and funding of individual- and community-engaged scholarship, practice, and policy.
At the federal level, there have been efforts to learn what would make it easier for the public to engage with the government to harness peoples’ “knowledge, needs, and lived experiences,” and federal entities like the US Food and Drug Administration (FDA) have developed new guidance, with broad input, related to engaging individuals and communities in their work (FDA, 2022). There are also agency-spanning efforts to better align federal actions that improve the vital conditions for health and well-being and empower communities to build resilience and achieve health equity (The Rippel Foundation, n.d.; Milstein et al., 2023).
In 2024, and for the first time ever, the National Institutes of Health (NIH), via its Community Partnerships to Advance Science for Society (ComPASS) program, provided research funding directly to community-based organizations to spark multisector, community-led structural intervention research (AAMC, 2024). Although the program recently concluded, ComPASS has built on similarly focused NIH efforts such as the NIH Community Engagement Alliance (CEAL) and the long-standing work of the Clinical and Translational Science Award (CTSA) consortium (NCATS, 2025; NIH CEAL, n.d.).
Since 2010, the Patient-Centered Outcomes Research Institute (PCORI), a publicly funded independent nonprofit, has advanced individual and community engagement through its funding of patient-centered comparative clinical effectiveness research. PCORI’s Engagement Award funding opportunities continue to support individuals and communities in building their capacity to understand, engage in, and disseminate research (PCORI, n.d.-a). Further, PCORI’s Foundational Expectations for Partnerships in Research provide baseline guidance on required elements of engagement PCORI funding applications (PCORI, n.d.-b). PCORI’s Advisory Panel on Patient Engagement, established in 2013, provides input on how to effectively engage communities, including developing Equity and Inclusion Guiding Engagement Principles (PCORI, 2023).
This federal work runs parallel to various philanthropic-funded efforts, often focused at the state or local level, to put individuals and communities at the center of evidence creation and policy translation (Everette et al., 2023; Engagement Scholarship Consortium, n.d.; Kresge Foundation, n.d.). On the ground and in the health care arena, there has also been a surge in “community-based providers” such as community health workers, promotoras, and navigators whose work aims to place patient experience, needs, and context at the center of the clinical relationship (Knowles et al., 2023; Madanat et al., 2023; Chan et al., 2023). Federal requirements for not-for-profit hospitals have seen health care organizations more deeply partner with their communities on needs assessments and community health interventions (Mathews et al., 2015; Cronin et al., 2024).
There have also been significant advances in guidance related to the development and assessment of individual- and community-engaged practices. The NAM’s Assessing Meaningful Community Engagement effort, which presents resources (a conceptual model, impact stories, and assessment instruments) to measure the impact of engagement, and PCORI’s Foundational Expectations are two examples (Organizing Committee, 2022). Further, the long-awaited third edition of the seminal text Principles of Community Engagement provides additional insight on how to deepen patient and community engagement in the development and implementation of programs, practices, science, and policies (CDC, 2024).
The Costs of Maintaining the Status Quo
Alignment in systems has a significant impact on outcomes. If a car wheel falls out of alignment, it strains the others, slows the vehicle, and makes the car difficult to steer. Misaligned pipes can restrict water flow. Invasive species can disrupt the delicate balance of roles and relationships in an ecosystem. Health sectors consist of complex systems with many interacting components (including patients, clinicians, researchers, market forces, social norms) and a range of competing or complementary goals. For example, the drive for revenue, profit, and investor returns might adversely affect other desired outcomes, like quality of care and access (Bellard, 2022; Edelman, 2025). Even when there are shared goals among these systems such as improving the health of the United States, policies, programs, and practices might not align with individual- and community-defined health goals and priorities. This lack of meaningful engagement and alignment results in significant and undesirable consequences at the professional, health, and economic levels, as described in this section. It is also important to note that there are also smaller-scale costs not detailed in this section, such as duplication costs and costs of short-term, siloed programs, that are critical to consider as they often underpin these larger-scale expenditures.
Economic Costs
Public and private resources that could be used to improve vital conditions, such as housing, early childhood education, and income support, compete and typically lose out to spending on reactive health care, health insurance, and downstream spending to mitigate issues like low rates of kindergarten readiness, child welfare interventions in the face of ill-health in parents or caregivers, and public safety and criminal justice spending on individuals primarily suffering from a behavioral health condition. Should health sectors steer toward maintaining the status quo, there are ultimately many negative economic financial implications at varying levels.
National health care expenditures reached $4.5 trillion (or $13,493 per person) in 2022, a 7.5 percent increase from the previous year (Martin et al., 2024). Expanding on this, waste accounts for nearly a quarter of health care spending (Shrank et al., 2019). Increasingly unaffordable health care has more Americans putting off care (61 percent of uninsured adults), not filling prescriptions (21 percent of adults), facing large debts (48 percent of insured adults), and worrying (73 percent of adults) (Lopes et al., 2024). Inequities in the US health care system cost an estimated $320 billion annually and could ultimately reach $1 trillion in spending by 2040 if they continue to be unaddressed (Bhatt et al., 2022).
Health Outcomes
As mentioned in the second section, when people seek health care system support, whether in diagnosing or managing disease or illness, there can be challenges in receiving care that aligns with their needs, circumstances, and personal preferences. This country’s focus and continually increasing spending on clinical care, which contributes just 20 percent to health outcomes, eclipses far lower investments in social and economic factors that are the largest contributor (40 percent) to how long and how well people live (County Health Rankings and Roadmaps, n.d.). However, in a study that explored the relationship between the ratio of social service (including housing, nutrition, and income support programs) to health care spending, states with a higher ratio of social to health spending had significantly better subsequent health outcomes across “adult obesity; asthma; mentally unhealthy days; days with activity limitations; and mortality rates for lung cancer, acute myocardial infarction, and type 2 diabetes” (Bradley et al., 2016, 760).
In addition, the conduct and publication of research have been increasingly directed toward biomedical research and its methodological strategies, despite the documented benefits of meaningfully engaging pressing issues as defined by individuals and communities served (Minkler and Wallerstein, 2008; Maurer et al., 2022; Sheche et al., 2024). For example, approximately 70 per-cent of the NIH budget was allocated to biomedical research in 2019 (Research!America, 2022). When individual and community goals and priorities are not the starting central reference points for which all health sector actions are authentically accountable, and when there is misalignment between these sectors and other systems that impact health, there can be a significant impact to disparities in disease prevalence, illness, and ultimately, population health outcomes (AHRQ, 2024a, 2024b).
While US life expectancy nearly returned to prepandemic levels in 2023, the life expectancy of comparable countries in the Organisation for Economic Co-operation and Development (OECD), which include Australia, Canada, Japan, Switzerland, the United Kingdom, and others, averaged nearly five years longer than the United States at 82.2 years (Rakshit and McGough, 2025; Wagner et al., 2024). This gap has widened further due to the COVID-19 pandemic. Compared to the OECD average, the United States also “has the lowest life expectancy at birth, the highest death rates for avoidable or treatable conditions, the highest maternal and infant mortality, and among the highest suicide rates” (Gunja et al., 2023). Within the United States, vast differences in life expectancy are also observed between census tracts or geographic areas (NCHS, 2020).
Professional Costs
Health sector professionals who are pressured to work within narrow definitions of health and adhere to requirements set by organizations or institutions—rather than being authentically accountable to the unique goals and priorities of individuals and communities—can face significant challenges. At the same time, it is imperative to provide health sector professionals and potential workforce partners closest to the issues with the time, resources, and training necessary to effectively address evolving needs of individuals and communities. Disregarding these critical factors can result in various costs, negatively impacting the health workforce as well as individual and com-munity trust and overall health.
Health care overall ranked last for employee satisfaction compared to 27 other industries, with 38 percent reporting risk of burnout (Burky, 2023). In one study conducted in June 2023 on job satisfaction and burnout among nurses and other health care workers, 91 percent of nurses and approximately one-third of physicians reported high levels of burnout, with some variation across hospitals and specialties (Galanis et al., 2023). Other research has surfaced that moral distress, a phenomenon that occurs when “one knows the right thing to do, but institutional constraints make it nearly impossible to pursue the right course of action,” can contribute to hospital staff burnout and be amplified by it, with depersonalization serving as a significant antecedent (Maunder et al., 2023, 2). Events recorded as frequently contributing to moral distress at a medium or high level included experiencing limited administrative support for a problem compromising patient care, inability to provide optimal care due to pressures from administrators or insurers to reduce costs or conduct unnecessary tests and treatments (Maunder et al., 2023). This aligns with other research showing that the prevalence of administrative tasks often results in delayed or forgone care, with approximately 24 percent of a sample of 4,155 respondents reporting such effects (Kyle and Frakt, 2021).
Solutions and Possible Gains
To overcome misalignment costs and help center the goals and priorities defined by individuals and communities in health sector actions and decisions, it is critical to identify potential solutions and corresponding levers that the nation can apply. Consideration of these solutions and levers will require health sectors to address the drivers of the problem and resulting challenges outlined earlier in the second section and summarized below.
Prominent Drivers
- Driver 1—Inclusive systems: There is a need for structures, procedures, and account-ability metrics that allow all individuals and communities to be authentically included and supported within and beyond the health sectors to advance meaningful engagement; meaning every person, in every community has the capacity to be authentically engaged in defining shared priorities and goals.
- Driver 2—Holistic health: There is a need for explicit adoption, use, and advancement of a holistic and comprehensive definition, under-standing, and operationalization of health, beyond a lack of physical disease.
- Driver 3—Multidirectional trust: There is a need for multidirectional trust, where health sector organizations demonstrate commitment and capacity and can reliably deliver on listening to, empathizing, and engaging with individuals and communities to continually demonstrate being trustworthy.
- Driver 4—Financial alignment: There is a need for a financial ecosystem that aligns the flow of money, resources, information, and prestige to individuals, communities, organizations, and institutions to best meet individual and com-munity health goals and priorities.
- Driver 5—Workforce capacity: There is a need for a health sector workforce that has the necessary tools and resources (such as training, time, funds, representation, and accountability metrics) to effectively engage with and be authentically accountable to individual and community health goals and priorities.
- Driver 6—Individual- and community-aligned evidence production: There is a need for data and evidence production, management, and sharing to be better leveraged and used by individuals and communities to achieve their goals and priorities and support continuous learning, including through research codesign and the cocreation of evidence.
Although certain systemic issues require intentional, sustained efforts over time, there are a range of policies, programs, and practices that can be leveraged in the near term to help support a reimagined health system that is aligned with and authentically accountable to individuals and communities. In this section, the authors provide a menu of four broad solution possibilities for achieving individual and community health goals and priorities, as well as corresponding cultural, legal, regulatory, and industry tools and resources activating meaningful change. The authors also present examples of successful programs and initiatives that have mitigated these drivers and issues, lessons learned, potential challenges for consideration, and possible gains from enacting the solutions. More levers and examples are also available for review and exploration in Appendix A.
Solutions
- Solution 1—Operationalize cross-sector holistic health and well-being: Establish and sustain a holistic perspective of health and well-being as modeled by the Vital Conditions Framework that requires all health sectors to adopt and contribute in ways determined through individual- and community-engaged processes. This holistic perspective on health and well-being includes effective prevention, diagnosis, treatment, and management of physical disease and the full spectrum of health—physical, mental, social and spiritual.
- Solution 2—Enact individual and community-accountable shared decision making tools and systems: Promote deeper collaboration and shared decision making among individuals, communities, and health sector institutions and organizations at local, state, regional, and national scales. Encourage authentic accountability of health sector resources, investments, and information flow to individual and community needs, goals, and priorities.
- Solution 3—Enact individual- and community-driven continuous learning processes: Invest in, test, and refine disaggregated, comprehensive individual- and community-driven research methods and research that are accountable to real-world health needs, goals, and priorities before generalizable knowledge This would encourage authentic data collection and evidence production and act as concrete strategies for advancing models of continuous learning across all health sectors accountable to individuals and communities.
- Solution 4—Invest in and sustain workforce capacity: Invest in training, support, and maintenance of a person- and community-centered workforce across all health sectors to achieve and be accountable to individual and community needs, goals, and priorities.
The solutions and levers surfaced in this section are supported by considerable evidence, but they are not mutually exclusive, and there is no shortage of potential starting points. It is also critical to note the underlying principles or elements (including radical empathy, as discussed in the introduction) that enable authentic implementation of the solutions and hold health sector institutions and organizations accountable for prioritizing individual and community health goals and priorities. Namely, the proposed solutions delineated below require that health sectors demonstrate they are worthy of their communities’ trust. It is impossible to meaningfully and effectively partner with individuals and community members as described if organizations have not shown they behave in ways that communities suggest reflect trust-worthiness; specifically, that means acting with respect, transparency, humility, and commitment, among other key behaviors (AAMC, n.d.; Chinekezi et al., 2023). Importantly, the AAMC Center for Health Justice found in a piloting of its Principles of Trustworthiness Toolkit that given their deep misgivings and mistrust, communities across the country were not willing to engage with health sector organizations in conversations about trust until they were able to “speak freely” about their experiences, histories, and perceptions. Listening, without rebuttal or interjection, and then reflecting together on what was heard and what lessons must be learned are the nonnegotiable first steps of this work (Alberti et al., 2025).
Mapping Solutions and Levers to Address Drivers
Solution 1
Establish and sustain a holistic perspective of health as modeled by the Vital Conditions Framework that requires all health sectors to adopt and contribute in ways determined through individual- and community-engaged processes. This solution may help address, in part, several underlying drivers: systemic barriers, a limited definition of health, the lack of multidirectional trust, misaligned financial incentives, and misaligned research. Possible levers to enact this solution include but are not limited to the following three levers:
- Lever 1: Fund, implement, and evaluate programs that support collaboration across all sectors relevant to the vital conditions to address both medical and nonmedical needs, with an emphasis on community-centered capacity-building efforts to enable a more community-led approach to addressing whole-person health and fostering community See Box 2 for an example.
- Lever 2: Implement and build on community information exchanges or SDOH information exchanges to optimize data collection and interoperability among the health sectors and other data systems to better address individual and community health goals. Depending on community capacity, resources, and goals, these community information exchanges and SDOH information exchanges can be regional or statewide.
- Lever 3: Create information technology systems that integrate and normalize data from multiple sectors to inform and support holistic care coordination, public health, and research—tracking data such as social needs, regional disparities, care journeys, access to services, and health outcomes—while leverag-ing responsible generative artificial intelligence to enhance data synthesis and Allow access to people within the community and other key stakeholder users to support robust communication and understanding across health sectors, individuals, and communities.
BOX 2 | Community Care Hub Example
A community care hub (CCH) is a “community-focused entity that organizes and supports a network of community-based organizations providing services to address health-related social needs” [a]. It centralizes administrative functions and operational infrastructure, fostering collaborations and ensuring services are accessible and culturally responsive [a]. The Administration for Community Living (ACL) helps build the conditions for CCHs to thrive through community infrastructure investments and programmatic and capacity building for CBOs that serve older adults and people with disabilities.
A prominent example of a CCH is the formation of the Partnership to Align Social Care (P2ASC), a national action and learning collaborative with strategic and operational workgroups represented by multiple sectors to align health and social care ecosystems. The P2ASC develops a wide range of practical tools and resources to implement newly aligned delivery systems of care and the emerging strategies to pay for social care in conjunction with health care [b].
SOURCES: [a] Pferr, L. 2023. Community Care Hubs: What evidence-based program providers need to know. Available at: https://www.ncoa.org/article/community-care-hubs-what-evidence-based-program-providers-need-to-know (accessed June 3, 2025). [b] Partnership to Align Social Care. n.d. About Partnership to Align Social Care. Available at: https://www.partnership2asc. org/about (accessed April 14, 2025).
Solution 2
Promote collaboration and shared decision making among individuals, communities, and health sector institutions and organizations at local, regional, and national scales. This solution may help address, in part, several underlying drivers: counteracting systemic barriers, a limited definition of health, the lack of multidirectional trust, misaligned financial incentives, and misaligned research. Possible levers to enact this solution include but are not limited to the following five levers:
- Lever 1: Use the Accountable Communities for Health (ACH) model to support transitioning from a centralized “power over” approach to governance and decision making to an individual- and community-driven “power with” mindset and ACHs are locally driven, multi-sector collaborations across community organizations, including public health, social services, and health care to address population health needs (Mittmann et al., 2022). See Box 3 for an example of an ACH.
- Lever 2: Build on promising practices, key insights, and lessons learned from Accountable Health Communities (AHCs), a model separate from ACHs, which was created by the Centers for Medicare and Medicaid Innovation (CMMI) and is one of the first federal initiatives to address SDOH at a national scale. This model tested “whether systematically identifying and addressing the HRSN of Medicare and Medicaid beneficiaries’ through screening, referral, and community navigation services will impact health care costs and reduce health care utilization” (CMS, n.d.). AHC also integrated community navigators into care coordination and care teams to ensure that patients were connected to culturally appropriate services and programs.
- Lever 3: Redesign funding structures and approaches to emphasize the importance of authentic engagement and aligning funding with individual and community priorities and goals. For philanthropy, this process could be supported by the continued movement toward trust-based philanthropy rather than approaches that assume philanthropic groups are worthy of trust. For federal funding (via the NIH, AHRQ, and others), this could take the form of shifting away from time-limited, outcomes-oriented granting mechanisms to providing funds that enable researchers to make long-term commitments to individuals and communities.
- Lever 4: Develop policies to improve data collection, analysis, and reporting of standards and processes at the state level to enhance health care, public health, and community collaborations.
- Lever 5: New collaborative models emerging in states, counties, and cities have created opportunities for citizens to have greater voice and power in making decisions on policy and budget priorities. Formal governance processes can embed structured community participation to shape policy design and decision making.
BOX 3 | Washington Accountable Communities of Health (ACHs)
Washington ACHs, led by Washington State’s Health Care Authority (HCA) and Medicaid Transformation Project, support the alignment of health and social care for Medicaid members, expansion of value-based care and outcome-based payment models, community alignment on shared health improvement priorities, and regulatory flexibility for cross-sector collaboration. Nine ACHs act as neutral conveners enabling place-based strategies for cocreating solutions with communities [a].
SOURCES: [a] Washington State Health Care Authority. n.d. Accountable Communities of Health (ACHs). Available at: https://www.hca.wa.gov/about-hca/programs-and-initiatives/medicaid-transformation-project-mtp/accountable-communities-health-achs (accessed April 14, 2025).
Solution 3
Invest in, test, and refine disaggregated, comprehensive individual- and community-driven research methods and research that are accountable to real-world health needs, goals, and priorities before generalizable knowledge requirements. This solution may help address, in part, several underlying drivers: systemic barriers, limited definition of health, a lack of multidirectional trust, and misaligned research. Possible levers to enact this solution include but are not limited to the following six levers:
- Lever 1: Create research infrastructure that explicitly shifts research efforts to recognize and encourage individuals and communities to take proactive roles in shaping the discussions and solutions for improving their health and well-being.
- Lever 2: Incentivize place-based approaches to identifying research questions and conducting research.
- Lever 3: Shift funding approaches to focus on long-term visions provided by individuals and communities versus short-term outcomes.
- Lever 4: Redesign research funding approaches to prioritize individual- and community-driven research, supporting researchers explicitly aligned with and seeking to advance individual and community health goals and priorities.
- Lever 5: Identify communities affected by the research topic and engage them in the design, conduct, and reporting of research, as well as in the dissemination and uptake of evidence. Resources cocreated by community and developed by PCORI-funded award teams include (1) Research Fundamentals: Preparing You to Successfully Contribute to Research (PCORI, n.d.-c), (2) Building Effective Multi-Stakeholder Research Teams (PCORI, n.d.-d), PCORI Compensation Framework (PCORI, 2015), Guide for Engaging with Research Partners About Data and Analysis (PCORI, n.d.-e), and Engagement Tool and Resource Repository (PCORI, n.d.-f).
- Lever 6: Emphasize authentic engagement in the conduct of CHAs, CHNAs, CHIPs, and other similar assessments that health and social service organizations are required to complete. These assessments should be conducted in collaboration with traditional health systems, sectors, and organizations, as well as those that impact health and address elements of the Vital Conditions for Health and Well-Being Framework. Such collaborations are not about simply completing a checklist item, but about fostering a continuous partnership in which historically underrepresented and marginalized individuals and communities and those with lived experiences have active roles in shaping the processes (including data collection, analysis, and implementation) and outcomes. Examples of these types of collaborations include the assessment executed by Delaware’s State Health Improvement Plan and the Columbia Gorge Community Health Needs Assessment in Box 4 (Delaware SHIP, 2025). A community-driven approach improves the utility of the CHA and implementation planning process by promoting greater integrity between community-identified health priorities and implementation strategies.
BOX 4 | Columbia Gorge Community Health Needs Assessment
Starting in 2013, a group of health care, public health, and social service organizations in the Columbia Gorge region spanning Oregon and Washington states assembled to accomplish a shared community health assessment (CHA) and community health improvement plan (CHIP) [a, b]. The collaboration made substantial innovations to what had previously been typical for these processes, especially the degree to which community members were included in both the assessment and improvement plan stages as well as the inclusion of groups surveyed. Prior to 2013, each organization executed their respective CHA and CHIP independently with limited outreach. As a result, there was no single comprehensive community health assessment for the region. The collaboration process was spurred by the establishment of the Columbia Gorge Health Council (the Health Council) as the governing entity for Medicaid in the region. The Health Council was required to complete a CHA/CHIP but saw an opportunity to pool resources and promote collaboration across disparate entities in the six-county region. Organizations participating in this collaboration included the Health Council, the region’s federally qualified health center, four hospitals, the public mental health agency, three health departments, and the Medicaid managed care organization.
The collaboration process drew heavily on the direction of individuals with lived experience who served on the Health Council’s Community Advisory Council, made up of Medicaid beneficiaries. Their role included consumer survey question review, addition, and modification; recruitment of focus group participants; and review and prioritization of results. In part due to the larger budget available once organizations pooled their resources, research-quality surveys with 65 questions were mailed with the final consumer survey to a simple random sample of 1,321 households in the Columbia Gorge region. In addition, community-based organizations hosted focus groups and hand-fielded surveys to allow the oversampling of populations experiencing barriers to health such as poverty, disability, or immigration status. Volunteers and staff visited places where hard-to-reach populations might be found and asked people to complete the survey. Of the 1,000 surveys printed for this purpose, 691 in-person surveys were completed, which yielded close to a 70 percent return rate [c]. A research organization affiliated with one of the health care systems compiled the results for the Community Advisory Council’s review [c].
The resulting CHA/CHIP reflected the priorities and needs of population groups within the region far better than what is typical for these processes, which can otherwise end up focusing more on market conditions, demand for services, and high-level demographics. The results also became a repository of information that was subsequently used for dozens of grant applications, which allowed for more efficient and effective application processes. The collaboration process has continued at three-year intervals as is required by the IRS of hospitals. However, in recent years, the number of organizations participating has grown from 11 to 19 to include other community-based organizations and the region’s United Way.
SOURCES: [a] Columbia Gorge Health Council. n.d. Learn more about the Community Health Assessment (CHA) and Community Health Improvement Plan (CHIP). Available at: https://www. cghealthcouncil.org/cha-chip (accessed December 19, 2025). [b] Columbia Gorge Regional Community Health Assessment. 2013. Columbia Gorge Regional Community Health Assessment. Available at: https://static1.squarespace.com/static/5e7109f83cff1b7d10e22da6/t/5e726c1 309d54f2db43c6b46/1584557083005/Columbia-Gorge-Community-Health-Assessment-December-2013.pdf (accessed December 19, 2025). [c] Stoneman, M., and M. McAninch. 2014. Providence Health & Services Oregon Region: 2013 Community Health Needs Assessments. Portland, OR: Providence Health & Services. Available at: https://www.providence.org/-/media/ Project/psjh/providence/socal/Files/about/community-benefit/pdfs/2013chnaandchipprovide nceseasidehospital.pdf (accessed February 25, 2026).
Solution 4
Invest in training, support, and maintenance of a person- and community-centered workforce across all health sectors to achieve individual and community needs, goals, and priorities. The authors anticipate that this solution would influence all targeted drivers. Possible levers to enact this solution include but are not limited to the following nine levers:
- Lever 1: Create organizational structures that serve to shift the culture of research toward one that values and prepares for authentic engagement. For example, this can be facilitated through practices such as fiscal readiness, institutional review board training to define and support the integration of community co-investigators, integration of engagement into promotion and tenure rubrics, and relationship building beyond grant funding.
- Lever 2: Fund community-based organizations and grassroots movements working toward building democratic, community-centered care Community-driven research initiatives advance democratic, community-centered care models by directing funding to com-munity-based organizations and grassroots movements that shape and lead the work (e.g., NIH’s ComPASS program and the American Heart Association/Robert Wood Johnson Foundation’s Health Equity Research Network focused on community-driven research).
- Lever 3: Encourage community navigator developed value plans to help effectively cap-ture health goals. These plans also empower community navigators to advocate for what matters most to At the state level, Medicaid or public health programs can sup-port the establishment of frameworks and distribution of funding to support community navigators in creating value plans.
- Lever 4: Fund and fairly compensate the active involvement of patients, communities, and those with lived experiences in health system navigation, advocacy, relationship building, and overall health This includes community health workers (CHWs), peer support specialists, promotoras, and more. Tying these models of care to financial reimbursement emphasizes the importance of longitudinal relationships, increases focus on prevention across the life course, and cultivates a kinship worldview. Many states are incorporating CHW services and unlicensed workers into value-based payment arrangements.
- Lever 5: Invest in researching, developing, and communicating the return on investment of burnout prevention for frontline health Use these insights to inform industry standards on wages, benefits, and working conditions that enhance staff retention.
- Lever 6: Establish and promote core competencies for frontline and supervisory workforce, prioritizing training in skills such as motivational interviewing, harm reduction practices, trauma-informed care, and authentic healing relationships (see Box 5 for an example).
- Lever 7: Explore accessible and interoperable technology-based strategies to reduce administrative burden on the workforce, creating more space and time for meaningful interactions with patients.
- Lever 8: Fund programs that incentivize individuals to pursue careers within health sectors, including scholarships, loan forgive-ness, and employment pathways with room for career growth.
- Lever 9: Facilitate educational and professional development opportunities within the workplace.
BOX 5 | Alaska Native Medical Center
The Alaska Native Medical Center (ANMC) is a nonprofit health center based in Anchorage, Alaska, and is one of several health care sites throughout the state that serve Native American or Alaskan Native (AI/AN) people. As recounted in her book, Thrive, Lisa Lawson, president and CEO of the Annie E. Casey Foundation, describes how this center provides an example of a health care system that positions people at the forefront, prioritizing interpersonal relationships and emphasizing preventive care to promote health and well-being (Lawson, 2025).
Despite being a large, integrated medical system, ANMC remains focused on the people they serve, referring to their patients as customer-owners. In practice, this means that patients are not treated as silent participants or subjects in decisions about their care; as the customer, they are the experts who know their goals and priorities best. For example, the health center has a traditional healing clinic where tribal doctors offer energy therapy, prayer, and dance, pairing the latest medical technologies with traditional native healing practices to ensure that their patient-customers receive the care they need and desire to be well. These tribal doctors are certified by an elder advisory council to ensure that their ancient practices continue through generations. While tribal doctors may provide recommendations for traditional medicine, the customer-owner is encouraged to discuss those recommendations with their primary care physician to ensure compatibility with any other medications included in their care plan. This is also an example of care that is wholly owned and directed by the patient as well as an example of how modern medicine can work in concert with ancient medicine. While engaging people served by health systems to help shape the way the systems operate is still a novel concept to some, embracing this practice might be what the health care system needs to be more effective and equitable (Lawson, 2025).
SOURCES: Lawson, L. M. 2025. Thrive: How the science of the adolescent brain helps us imagine a better future for all children. New York: The New Press.
BOX 6 | Wellville Example
For example, in the Wellville community of Spartanburg, South Carolina, a group of stakeholders came together to launch Hello Family, an alliance of over 60 partnered organizations providing a continuum of evidence-based services to young children and their families, free of charge to all city residents [a]. The initiative is producing community-wide improvements in neonatal intensive care unit admissions, full-term births and healthy birth weights, among other measures [a, b]. It is also a model for aligning goals, investments, and systems. Program providers, investors, government, and other stakeholders are connected through a set of shared outcomes, and the effort is financed through an innovative pay-for-success strategy [c]. Following its initial success, Hello Family is now being expanded to the entire county [d].
SOURCES: [a] Brush, R. 2025. Change from within: A 10-year journey to improve health in five Wellville communities. Paper presented at Connecticut Children’s AY25 Pediatric Grand Rounds Honorary Dworkin Lecture, January 14, 2025, Hartford, CT. Available at: https://wellville.net/ wp-content/uploads/2025/02/Change-from-Within_Presentation-on-January-14-2025.pdf (accessed February 25, 2026). [b] Boroughs, B. 2024. How partnerships between organizations can transform a community for the better. Newsweek, March 13. Available at: https://www.newsweek. com/how-partnerships-between-organizations-can-transform-community-better-1878412 (accessed June 2, 2025). [c] Sandstrom, H., W. J. Congdon, M. Zhong, and F. Hernandez-Lepe. 2024. Spartanburg Hello Family Pay for Success Project Evaluation Design. Washington, DC: Urban Institute. [d] City of Spartanburg. 2024. Hello Family shares transformative results, expands countywide. Available at: https://www.cityofspartanburg.org/CivicAlerts.aspx?AID=71 (accessed April 14, 2025).
Projections of Possible Gains from Enacting the Solutions
There are substantial potential benefits to greater alignment of goals among those in the health sectors and the individuals and communities they serve. Specific examples to illustrate what is possible today include the following outcomes.
Individual Outcomes
A recent study on physician altruism—defined as “putting the patient first”—found that doctors who prioritize patient care over income and profit achieved dramatically better health outcomes with Medicare patients (Casalino et al., 2024). These positive outcomes observed in the study included 38 percent fewer potentially prevent-able hospitalizations; 41 percent fewer potentially preventable emergency room visits; and 9 percent lower annual medical expenses (Casalino et al., 2024). The study concluded that “policymakers and leaders of hospitals, medical practices, and medical schools may want to consider creating incentives, organizational structures, and cultures that may increase, or at least do not decrease, physician altruism” (Casalino et al., 2024, 1). In addition, studies show that patients who feel acknowledged, value their relationship with, and trust their health care provider are more likely to express satisfaction with their health care experience, even if their clinical care goals are not ultimately realized (Chipidza et al., 2015; Birkhäuer et al., 2017; ChenMed, 2024).
Community Outcomes
On a broader scale, the health of people living in a geographic area depends to a large degree on the collective decisions, actions, and investments of stakeholders that affect the conditions of those communities (Center on Social Disparities in Health, Build Healthy Places Network, and Robert Wood Johnson Foundation, 2015). National initiatives like Wellville (see Box 6), BUILD Health Challenge, Invest Health, and Purpose Built Communities have supported hundreds of multisector partner-ships in communities that are bringing people and organizations together around shared interests and pointing the way to more effective, more equitable, and more sustainable approaches to health and well-being. Learning from these community health collaboratives can illuminate the barriers and enablers of aligning across stakeholders (Brush, 2024).
As noted in the lever examples, the ACH model and other models are also exploring how collaboration and shared decision making can improve health outcomes and lower health care costs. In Connecticut, an actuarial study on the state’s proposed Health Enhancement Community model estimated potential 10-year savings from prevention of $1.37 to $3.26 billion for Medicare, $1.1 to $1.9 billion for Medicaid, and $1.8 to $2.3 billion for commercial payers (Connecticut Office of Health Strategy, 2019). Achieving these savings would require health sector alignment, coordinated action, and substantial long-term investment in the vital conditions needed for health (The Rippel Foundation, n.d.).
Societal Outcomes
The biggest gains from an aligned and authentically accountable health system with individual and community health goals and priorities would occur at a national level. A healthier population is more productive, spends less on health care, and enjoys a higher quality of life (HHS, 2021; Center for Health Incentives and Behavioral Economics, 2017; OECD, n.d.). According to a recent economic analysis by Deloitte Center for Health Solutions, improving health equity nationwide could add $2.8 trillion to the US gross domestic product by 2040, increasing profits of US-based businesses by an estimated $763 billion in the same time period (Gebreyes et al., 2024).
Choosing a Path Forward
Ultimately, greater alignment with individual and community health goals and priorities requires agreement on desired outcomes, the line of sight on how to get there, and accountability for results, including changing course when necessary. System dynamics models like the Thriving Together model can simulate possible futures depending on how stakeholders prioritize investments in community health (Milstein et al., 2022). Recognizing that there are many options for investing in community health, the Thriving Together model tested various allocations of investments across four assets:
- Urgent services capacity (e.g., acute care for injury or physical/mental illness),
- Vital conditions (housing, transportation, learning, work and wealth, and more),
- Equity (measured by how fairly income is distributed), and
- Belonging and civic muscle (based on social associations per capita).
After running various scenarios, the authors conclude that “The best resilience strategy may require decisive shifts from historical priorities…investing early in both equity and belonging and civic muscle so that one may build on those assets later: a kind of self-reinforcing, asset-building maneuver” (Milstein et al., 2022, 8). They also note that “It takes dedicated resources to establish greater interdependence and enable stewards to work across differences, devise shared plans, gather and manage assets, and adapt to challenges over time” (Milstein et al., 2022, 8).
Marshaling the Momentum Toward Change
Our economy is rooted in scarcity, competition, and the hoarding of resources, and we have surrendered our values to a system that actively harms what we love . . . [We need] another model. . . where wealth and security come from the quality of our relationships, not from the illusion of self-sufficiency . . . All flourishing is mutual. (Kimmerer, 2024, back cover)
There may be an effective and affordable way to unlock much greater health and economic potential, ultimately reducing severe illness by 20 percent, lowering health care costs by 14 percent, and improving economic productivity by 9 percent . . . The question remains whether there are, in fact, U.S. regions where a critical mass of organizations are committed to make such investments together. (Homer et al., 2016)
Redefining Accountability
These two quotes distill theories of change for building momentum to advance the solutions and levers described toward real-world change. First, Kimmerer’s words, “All flourishing is mutual,” emphasize the importance of recognizing that true wealth and security arise from the quality of relationships, rather than the illusion of self-sufficiency (Kimmerer, 2024, IX). Second, Homer and colleagues’ quote emphasizes the importance of regional, collective action to cultivate real-world improvement in health and economic outcomes (Homer et al., 2016). In alignment with the intro-duction of this discussion paper, building the momentum for this type of change requires a shift in accountability approaches.
Traditional approaches often only rely on procedural accountability, which uses incentives or punishments to drive behavior (Hunter, 2024). While this approach has value, it is often a shallow form of accountability, in that it relies on people to “do the right thing” because of rewards or punishments only and can therefore be viewed as an insufficient “Band-Aid” to advancing authentic accountability when used alone. A complementary approach would be what the authors label as caring accountability. Caring accountability arises when individuals, communities, organizations, and sys-tems recognize their inherent interconnectedness and interdependence and feel drawn to fulfill their responsibilities out of mutual benefit and reciprocity, which aligns with Kimmerer’s quote.
Two key changes are critical to enable this shift in accountability. First, there is a need for a cultural shift in mindset from one guided by scarcity and the illusion of independence to one that centers the quality of relationships between individuals and communities and the organizations and systems meant to serve them. This shift in mindset can incorporate both caring and procedural account-ability to help achieve authentic accountability. There are many starting strategies and resources to support this shift, including those embedded in the solutions and levers mentioned in the previous section, as well as others that can help explore the inherent interconnectedness of people and systems (including The Consilience Project); identify and address scarcity mindsets; and reinforce practices of gratitude, reciprocity, and interdependence (The Consilience Project, n.d.; Klein and Thompson, 2025; Scharmer and Senge, 2016).
Second, it is important to note that this shift in accountability is often more feasible to execute at smaller, regional scales to enable health sectors to prioritize individual and community goals and priorities (Mittmann et al., 2022). A regional scale, whereby it is large enough to foster some degree of self-sufficiency and small enough to enable authentic care-driven accountability, emerged as a critical scale within Homer et al.’s simulation work (Homer et al., 2016). By placing quality relationships at the center, regional health sectors and other key players, such as those well-equipped to advance the vital conditions, can collaborate effectively to implement the four solutions described in the previous section, tailoring their efforts to the specific levers and strategies that work best within their unique context.
Thus, building the momentum for real-world change necessitates bottom-up driven innovation that centers authentic, mutually beneficial relation-ships. Rather than solely enacting change from the “top-down” (e.g., through federal mandates), local actors, including within states, towns/cities, and counties, must be supported and empowered to work together at an explicitly regional scale. By combining authentic accountability and leveraging a bottom-up approach, momentum can be built over time via a strong emphasis on two key points:
- Leveraging the unique assets, strengths, cultures, and challenges of different groups to develop locally appropriate solutions. While these solutions may look different from one place to the next, they can still be guided by underpinnings of the four solutions (Terrana et al., 2024).
- Leveraging local, state, and regional philanthropy, government, and their partnerships to create and sustain the momentum needed for local real-world change. This would include communicating and coordinating with one another so the diffusion of innova-tion can spread to other regions over time, and every individual and community can benefit from the resulting change (Bloomberg Philanthropies, n.d.).
However, there are two critical challenges that must be addressed. First, it is often not in an individual’s or organization’s best interests to change if they are acting alone, despite a collective recognition of the problem. This requires a commitment to collective action and a willingness to work together to overcome the status quo. Second, there is a need for robust and sustained long-term investments in regional groups capable of enacting the proposed solutions synergistically. This requires a commitment to investing in the capacity and infrastructure of regional health sectors as well as a willingness to take a long-term view and prioritize the well-being of individuals and communities over short-term gains.
Addressing the Need for Collective Action
The concept of a Nash equilibrium, derived from game theory, offers a plausible framework for understanding the allure of the status quo. A Nash equilibrium occurs when no individual actor can improve their outcome by enacting change alone, assuming all other actors maintain their current approach. This phenomenon is evident across the health sectors.
In the health care industry, systems often rely on tertiary and quaternary care to generate prof-its, often at the expense of primary care, which frequently results in financial losses. If one health care system were to shift its business model, such as transitioning to value-based care, it would likely place itself at a competitive disadvantage compared to other systems that continue to profit from tertiary and quaternary care. Within public health systems, a strong emphasis is placed on core mission areas, such as vaccine administration, chronic disease prevention, and surveillance, as these activities can be used to demonstrate the value and return on investment of public health initiatives. However, this narrow focus often leads to underinvestment in cultivating belonging, civic muscle, and community capacity despite the long-term recognition of the importance of this role and the potential for long-term benefits, as suggested by the Thriving Together model (Kesler, 2000; Milstein et al., 2022). If public health departments were to unilaterally shift their investments toward fostering these components, they would likely experience a short-term decline in the metrics used to justify their funding, thereby increasing the risk of losing taxpayer support. Finally, the health science enterprise is constrained by its current incentive structure, which prioritizes the production of general knowledge over taking part in continuously LHSs that are aligned with using data and evidence to improve local conditions first over general knowledge production. As a result, researchers who focus on advancing general knowledge are often rewarded with resources, information, and prestige, while those who prioritize local improvement may see their careers diminished (Hoppe et al., 2019).
Overall, this creates a challenging environment for health sector actors, who, despite their good intentions and awareness of the problems, become trapped in a Nash equilibrium that is difficult to escape. Thankfully, there are precedents and concrete examples that can inform local, state, and regional efforts to break this equilibrium (Ostrom, 1990; Metcalf and Casey, 2016). Effective strategies for escaping a Nash equilibrium include the following:
- Emphasize communication and coordination among actors to promote a unified
- Establish explicit agreements that enable all actors to change their strategies
- Implement enforcement mechanisms to pre-vent individuals from reverting to old strategies for personal gain.
- Foster trustworthy relationships and recognize the long-term interdependence among actors.
- Modify the “rules of the game” by enacting new policies at the local, state, regional, and federal levels to shift incentives and structures in support of the new approach.
- Provide leadership support and transfer power to leaders who are best equipped to drive change and break the Nash equilibrium.
By adopting these strategies, health care, public health, and health science enterprise actors can work together to escape the constraints of the cur-rent Nash equilibrium and create a more equitable and effective health landscape.
Addressing the Capability Trap
A second challenge to achieving robust change is the “capability trap,” a phenomenon where an organization or system becomes stuck in a cycle of poor performance due to a focus on short-term fixes rather than investing in core capabilities necessary for long-term success (Landry and Sterman, 2017). This cycle is characterized by a focus on immediate needs, leading to a depletion of resources and erosion of core capabilities over time. A notable example of this occurred during the COVID-19 pandemic, where health care professionals were overworked and under-resourced, leading to burnout and workforce attrition.
While this is an acute example, this challenge is pervasive and a likely partial explanation for many of the high costs described in the third section of this discussion paper, manifesting in a variety of ways. For example, Landry and Sterman highlight how the health care system could be viewed as the “short-term solution” that draws resources from other sectors, such as the public health system and sectors responsible for the other vital conditions of health (Landry and Sterman, 2017). With this, funds flow to treatment instead of prevention and investments that could enhance community capacity. This same dynamic is observed in the funding portfolio of the NIH. In 2019, 70 percent of the NIH’s extramural budget was dedicated to biomedical research, with an estimated 22 percent dedicated to social and behavioral research and 8 percent to environmental research (Hekler et al., 2022). Prior estimates suggest biological determinants explain 30 percent of the variance of health outcomes, whereas other factors, such as social, behavioral, and environmental factors, explain the remaining 70 percent of variance (McGinnis et al., 2002). Thus, the funding portfolio of the NIH could be viewed as manifesting a capability trap, whereby the short-term biomedical solutions are invested in at the expense of robust investments in other determinants of health (Kaplan, 2019; Hekler et al., 2022). This is a trap within the health science enterprise as, at this point, the advanced biomedical solutions are needed to address the diseases that manifest from, in part, the unhealthy social, behavioral, economic, and ecological conditions present in the United States.
However, there are strategies to overcome the capability trap. One key lesson is that when working to overcome the trap, things may initially worsen before improving. For instance, a health care executive may need to allocate resources to develop sustainable local solutions, which could lead to a temporary decrease in patient through-put. However, this investment can ultimately empower clinicians to address the root causes of problems and improve the overall capabilities of the system. This approach is an example of strategic capability development. Other effective strategies for overcoming the capability trap include the following:
- Target root cause issues to guide collective action and target investments toward explicitly counteracting a capability trap (e.g., the ReThink Health model) (Milstein et al., 2025).
- Realign incentives to encourage investment in core capabilities.
- Shift mindsets and culture to prioritize long-term success over short-term gains.
- Implement process improvement initiatives to enhance continuous learning processes, including the Learning Health System Shared Commitments (McGinnis et al., 2024).
- Adjust monitoring and evaluation approaches to track dynamic issues and changes rather than assuming linear developments.
- Invest in all capabilities, including metrics, IT systems, and workforce upskilling in process improvement and learning (Landry and Sterman, 2017).
Regional groups working to drive change can draw on these strategies and insights to overcome the capability trap and achieve robust, sustainable improvements aligned with individual and community health goals and priorities. By acknowledging the challenges posed by the capability trap and adopting a strategic approach to capability development, the health sectors can break free from the cycle of poor performance.
Summary
In summary, the US health sectors, including health care systems, the health science enterprise, and public health systems, often fail to prioritize the perspectives of individuals and communities, instead relying on paternalistic approaches that neglect the importance of community expertise and input. A health care system that delivers effective, equitable, and sustainable care, a public health system that cultivates belonging and civic muscle, and a health science enterprise that advances an actionable research agenda driven by individuals and communities are essential for achieving optimal health and well-being for individuals, communities, and broader society.
Achieving health sectors that prioritize individual and community health goals and priorities requires a multifaceted approach that addresses six underlying, interconnected drivers of the problem. Ultimately, the goal is to foster health for everyone, in every community via health sectors that align with the goals and priorities defined by individuals and communities. This involves a fundamental transformation in the way health sectors approach their work, and a commitment to establishing trust, advancing radical listening, empathy, and bidirectional learning with the people they serve. By working together to achieve this vision, a healthier, more equitable, and more just society for all is possible.
Appendix A
The authors raised and discussed additional levers and examples that were not incorporated into the section on solutions and possible gains to focus on priority options. In addition, there were some possibilities not explored in depth by the full author group. To retain all possible ideas and provide a springboard for further exploration of relevant priority actions, the authors organized them into this appendix for review by relevant audiences.
Levers for Further Exploration Across Solutions
Solution 1—Operationalize Cross-Sector
Holistic Health and Well-Being
- Scale and spread multisector partnerships and collaborations that center the goals of individuals and communities in advancing the vital conditions, shifting to a model of collaboration in which authentic, reciprocal relationships are in sync and balanced, referred to as Collective Impact 3.0 by the Tamarack Institute (https://www.tamarackcommunity. ca/articles/collective-impact-3.0-an-evolving-framework-for-community-change).
- Create mechanisms for community-based organizations to tap into health care dollars, including through 1115 waivers, community care hubs, and multiyear funding streams inclusive of research and evaluation budgets.
- Use elements of widely recognized frameworks and benchmarks at the national and global levels, such as the U.N. Sustainable Development Goals Model (https://www.org/sustainabledevelopment/) and Healthy People 2030 (https://odphp.health.gov/), to provide guidance on advancing population health, equity, and well-being.
- Implement policies to include nonprofit hospital standards under the IRS, state laws, and conditions of participation for Medicare.
Solution 4—Invest in and Sustain Workforce Capacity
- Eliminate requirements of college degrees for entry-level roles and facilitate educational and professional development opportunities within the workplace.
- Elevate the role of the community workforce by formalizing affordable educational pathways through community and four-year colleges, as well as professional certifications.
- Acknowledge the value of the workforce by raising the visibility and prestige associated with these career paths.
- Destigmatize addiction, disability, aging, and mental health and other chronic diseases to attract more professionals to work with these populations.
Additional Examples to Model
Solution 1—Operationalize Cross-Sector Holistic Health and Well-Being
- The Federal Plan for Equitable Long-Term Recovery and Resilience (ELTRR) (https:// rippel.org/vital-conditions/) has provided a comprehensive vision and detailed plan to align investments, policies, and It could be leveraged to gain sufficient background on a comprehensive perspective on health, its impacts, and examples for how to foster more robust cross-sector coordination and collaboration. This plan has explicitly empha-sized centering belonging and civic muscle, otherwise known as robust democratic pro-cesses that establish systems accountable to individual and community goals and priorities.
- Through the US Department of the Treasury’s Social Impact Partnerships to Pay for Results Act (SIPPRA) (https://home.treasury.gov/ services/social-impact-partnerships/sippra-pay-for-results), the federal government makes payments to state and local projects that “demonstrate measurable outcomes in areas such as reduced homelessness and improved children’s health while reducing governmental costs. By leveraging data and evidence-based practices, the SIPPRA program seeks to empower communities and improve the quality of life for those in need” (US Department of the Treasury, 2024).
- Under the Affordable Care Act (ACA), the Family and Community Engagement Initiative (CEI) (https://californiaengage.org/) encourages health care providers to engage partners outside of the health sectors, such as schools and faith-based organizations, to enhance the health and well-being of children and families in One of the ways CEI encourages this type of engagement is by providing relationship builders and peer-to-peer partnerships aimed to strengthen community engagement. The ACA can support similar activities to promote collaborative efforts through programs funded by the CMMI.
- Funding models such as outcome-based financing, pooled funding, and braiding funding streams can be used to combine resources from public and private sectors to address multiple health drivers simultaneously. For example, California Advancing and Innovating Medi-Cal (CalAIM) employs a combination of braided funding and outcome-based financing to integrate California’s Medi-Cal program more seamlessly with other social services. CalAIM’s community support (CS) services enable Medi-Cal managed care plans to pay for nonmedical services, such as housing supports, food assistance, and personal Providing Access and Transforming Health enables health care entities to directly contract with community-based organizations to provide CS and enhanced care management, encouraging meaningful community engagement.
- CommonSpirit Health’s Research and Equity Advisory Council for Housing Insecurities (REACHI) nurtures partnerships between the health care system, providers of homeless services, and people with lived experience of homelessness. REACHI prioritizes REACHI members’ preference for logistic and informational support (e.g., location, timing, method of meeting) and fair compensation for time and engagement.
- A transformed care continuum for complex and highly expensive patients is necessary, including those residing in skilled nursing facilities. Whether patients go to a skilled nursing facility or their home, many need brief evidence-based coaching to build their own self-care skills and resources. Postacute social care providers can support patients identified as high risk for readmission with a focus on assuring a safe environment, ensuring appropriate food is available, and reviewing medications for safety and a system for taking them properly. Longer, ongoing social care coordination provided in conjunction with medical care and community care specialists has emerged as key to success for individuals with more complex care and support needs.
- University-wide (as opposed to strictly medical school- or public health school-wide) training on the social drivers of and multisector contributions to health should be implemented.
- The U.S. Playbook to Address Social Determinants of Health (SDOH) was published in 2023 to reimagine new policies and actions around SDOH, including examples and guidance on collaboration inside and outside of government.
- An example of a health and community information exchange to potentially model includes the San Diego County Community Information Exchange (https://ciesandiego. org/san-diego/).
- The Fox Valley Data Exchange (https://cffoxvalley.org/loop/2024/10/21/powerful-new-data-platform-launched-for-tri-county-region/) is an example in eastern Wisconsin that combines data from more than 30 sources to provide aggregated data aligned with the Vital Conditions Framework for community planning and decision
Solution 2—Enact Individual and Community-Accountable Shared Decision Making Tools and Systems
- In California, state government leaders have leveraged several legal and policy levers to improve standardizing the collection of data, as well as new reporting and sharing requirements. The levers used include setting new standards and practices through required federal reporting processes from the Centers for Medicare and Medicaid Services (CMS); using legislative and regulatory processes for new data measures; and including required practices into memoranda of understanding or service contracts. Through enacted legislation (AB 133), California created the Data Health Exchange Framework, a multiagency effort to share information using standard categories including HRSN, disability/ability status, tribal affiliation, and more. The legislation authorizes the agency that licenses health plans, California’s Department of Managed Health Care, to establish health equity quality measures and benchmark standards for all health plans licensed by the agency. This direction allows for performance measures and standards across commercial and government-sponsored health plans. The legislation also authorizes the creation of a committee to make recommendations to the agency composed of representatives from government agencies, health care industries, and representation and knowledge of California’s diverse com-munities. Related to these efforts, the state’s Medicaid agency, the Department of Health Care Services, leveraged an administrative process—its regular reporting requirements to CMS—to update its Comprehensive Quality Strategy, requiring health plans offering coverage both through the state health exchange, Covered California, and its Medicaid program, Medi-Cal, to stratify and report quality performance measures by race and ethnicity. These requirements are included in the service contracts that the state and health plans enter with the respective state agencies.
- Participatory budgeting (https://www.participatorybudgeting.org/), citizens’ assemblies ( https:// www.newyorker.com/news/the-lede/what-could-citizens-assemblies-do-for-american-politics), and mayoral coordination—as advanced in the Bloomberg Sustainable Cities Initiative—serve as opportunities for citizens to have greater voice and power in making decisions on policy and budget priorities.
- The National Academy for State Health Policy’s Healthy People, Healthy States: Promising Practices to Address Health Disparities Toolkit (https://nashp.org/ healthy-people-healthy-states-promising-practices-to-address-health-disparities/) emphasizes community representatives in committees to structurally play a role in the design and governance of state policies.
- The Connecticut Office of Health Strategy and the Department of Public Health created a comprehensive proposal for Health Enhancement Communities (HEC) (https://portal.ct.gov/ohs/-/media/ohs/hec/ct-sim-hec-framework-technical-report.pdf) by soliciting input from a diverse group of stakeholders representing individuals, communities, and health sectors. The HEC framework demonstrates the value of investments in long-term efforts of multisector collaboratives to improve community conditions needed for health. Elements of this proposal are now being considered for state Medicaid reform.
- The California Endowments “Building Healthy Communities” initiative (https://www. calendow.org/learning/executive-summary/) is an example of engaging individuals and communities in advocating for change, creating a sense of agency that promotes health in ways that prescriptive interventions cannot.
- Patients 4 Primar y Care (https://p4pc.org/) organized to advance the patient and community voice in policy and other realms in support of making primary care a national priority.
- A National Academies publication, Community Power in Population Health Improvement: Proceedings of a Workshop (https://nap.nationalacademies.org/catalog/26306/ community-power-in-population-health-improvement-proceedings-of-a-workshop), explores issues related to community-driven power-building efforts to improve population health.
- Young Invincibles (YI) (https://younginvincibles.org/) is an organization that was founded by a group of students in the summer of 2009, motivated by the recognition that young people’s voices were not being heard in debates over health care reform. Over the past 15 years, YI has expanded from a group run out of a school cafeteria to a national organization with offices around the country, taking on issues related to health care, higher education, and economic security. They are committed to expanding opportunity and access for young adults ages 18 to 34 and making sure those individuals’ perspectives are heard wherever decisions about their collective future are being made.
- Age-Friendly Health Systems (https://www. ihi.org/partner/initiatives/age-friendly-health-systems) is an initiative of the John A. Hartford Foundation and the Institute for Healthcare Improvement, in partnership with the American Hospital Association and the Catholic Health Association of the United States. The initiative launched to build a movement toward age-friendly care delivery that is evidence based, causes zero harm, and aligns with what matters most to older adults (the US population aged 65+) and their family caregivers. Their underlying framework (What Matters, Medication, Mentation, and Mobility) was foundational for the development of a new Age-Friendly Hospital Measure introduced by CMS in 2025.
Solution 3—Enact Individual and Community-Driven Continuous Learning Processes
- The SCAN Foundation’s investment in “United for Health Equity in Aging” has heavily impacted the approach to addressing health inequities in older adults. The initiative emphasizes the importance of combining traditional health data with personal stories to address health inequities and advance social justice, empowering communities to explore and decide the best action steps to addressing health disparities in older adults. Additionally, SCAN Foundation partnered with the Public Policy Lab to build The People Say, a first-of-its-kind resource and catalog of older adults’ experiences that helps policy makers hear the voices of older adults when crafting policies.
- Following the exemplar set by the Congressionally Directed Medical Research Program, every application for PCORI community-engaged research funding is reviewed by two scientists or researchers, one patient representative, and one representative of the broader health care community. As with the application review process, PCORI peer review also engages patients and represen-tatives of the broader health community.
- In Hartford, Connecticut, the North Hartford Triple Aim Collaborative is leading efforts by three hospitals and the city’s Health and Human Services department to source a shared set of data, engage community members in providing resident perspectives, and align priorities and potential coinvestments.
- In Spartanburg, South Carolina, the Live Healthy Spartanburg Collaborative (https://livehealthyspartanburg.org/) engaged grassroots and community organizations across the county and conducted resident listening sessions to add depth and real voices to the qualitative component of Spartanburg Regional Health System’s 2024 CHNA.
- The work of Generation Patient (https://generationpatient.org/) serves as an example of a group promoting clarity on health care system needs and challenges and organizing for advocacy to prompt legislation that advances health, well-being, and equity. It is a widely recognized issue among young people living with chronic and rare health conditions that social media feeds often present a barrage of misinformation and misleading content about the prescription drugs they desperately need to live full and healthy lives. In recent years, young people have been left on their own to sort through information that is designed to take advantage of their vulnerabilities. Generation Patient, along with the Young People’s Alliance and the US Public Interest Research Group, engaged the FDA on this issue, eventually leading to the introduction of the Protecting Patients from Deceptive Drug Ads Online Act, which directs the FDA to update and enforce regulations for how prescription drugs are marketed on social media.
Solution 4—Invest in and Sustain Workforce Capacity
- PCORI intentionally seeks diverse, iterative input through a variety of modalities, such as convenings and asynchronous input PCORI applies “fit-to-purpose” strategies, conducting careful landscape and feedback analyses to foster representation in their work. PCORI also integrates individual and community voices into its programmatic activities using advisory panels. These panels represent a diverse cross section of the broader health and health care community and serve as longitudinal bodies providing insights into broad areas of focus. Their contributions include offering perspectives on refining funding approaches and improving methods for engaging patients as research partners.
- The Pathways Community HUB Institute (PCHI) (https://www.pchi-hub.org/our-model) provides a framework for communities to build sustainable community care coordination networks with CHWs employed by CBOs. Through outcome-based payments, Pathway Community HUB entities provide direct contracting between CBOs with CHWs and health care organizations, allowing greater stability of CHWs based in community settings.
- Oregon Health Authority (https://www.oregon.gov/oha/HPA/dsi-tc/Documents/THW-Payment-Model-Guidance.pdf) established a certification and registration process for CHWs, peer support specialists, and doulas, among Their registration standards and state involvement allowed for the identification of unlicensed individuals working in specific capacities the ability to enroll as Medicaid providers and bill their services under the Oregon Health Plan.
- In 2023, Senate Bill 117 (https://nashp.org/ state-tracker/state-community-health-worker-policies/nevada) was introduced in Nevada, allowing Nevada Medicaid to expand flexibility for where CHWs can provide services (including community settings) and empowering CHWs to bill without physician Prior to 2023, CHWs were required to work under the direct supervision of a physician or other licensed health care provider to receive reimbursement. This change promotes the autonomy of CHWs and allows them to play a more prominent role in delivering services, particularly in underserved or rural areas.
- Texas’s peer support specialist, promotoras, and behavioral health workforce initiatives and New Mexico’s promotoras training and integration into the public health system sup-ports community needs by involving individuals with lived experiences in the provision of care, helping to reduce stigma and increase engagement with health and public health services.
Resources to Promote Learning and Conversation
Resources that Promote Thinking Around Caring Accountability
- Planetary Boundaries (https://www.stockholmresilience.org/research/planetary-boundaries.html)
- Braiding Sweetgrass (https://milkweed.org/ book/braiding-sweetgrass)
- Restoring the Kinship Worldview (https://www.com/books/690771/ restoring-the-kinship-worldview-by-wahinkpe-topa-four-arrows/)
- Abundance and Reciprocity in the Natural World (https://birchbarkbooks.com/products/ the-serviceberry)
Resources for Truth and Reconciliation Commissions
(Truth and reconciliation commissions are bodies that investigate patterns of abuses of human rights or humanitarian law committed over a number of years, concluding their work with findings and recommendations.)
- Truth and Reconciliation Commission of Canada (https://nctr.ca/about/history-of-the-trc/truth-and-reconciliation-commission-of-canada/)
- The California Reparations Report (https://oag.gov/ab3121/report)
- Fostering the Civil Rights of Health in the context of COVID-19 (https://static1.squarespace. com/static/5956e16e6b8f5b8c45f1c216/t/6 064ad55bada160fe923507b/1617210710027/Chp 37- Harris _COVIDPolicy Playbook-March2021.pdf)
Resources for Advancing a Health Justice Framework
- Health Justice: A Framework (and Call to Action) for the Elimination of Health Inequity and Social Injustice (https://digitalcommons.wcl.edu/cgi/viewcontent.cgiarticle=2125&context=aulr&ref=pagingfuturedocs.com)
- Health Justice Strategies To Combat COVID-19: Protecting Vulnerable Communities During A Pandemic (https://www.healthaffairs.org/content/forefront/health-justice-strategies-combat-covid-19-protecting-vulnerable-communities-during)
- Health Justice Strategies to Combat the Pandemic: Eliminating Discrimination, Poverty, and Health Disparities During and After COVID-19 (https://papers.ssrn.com/sol3/ cfm?abstract_id=3636975)
- The Civil Rights of Health: A New Approach to Challenging Structural Inequality (https://www.org/the-civil-rights-of-health-a-new-approach-to-challenging-structural-inequality/)
References
AAMC (Association of American Medical Colleges). 2024. Community partnerships to advance science for society: An NIH-Wide effort for health equity. Available at: https://www.aamchealthjustice.org/news/viewpoint/nih-compass-program (accessed June 3, 2025).
AAMC. n.d. The Principles of Trustworthiness Toolkit.
Available at: https://www.aamchealthjustice.org/ key-topics/trustworthiness/trustworthiness-toolkit (accessed November 4, 2025).
Abernethy, A., L. Adams, M. Barrett, C. Bechtel, P. Brennan, A. Butte, J. Faulkner, E. Fontaine, S. Friedhoff, J. Halamka, M. Howell, K. Johnson, P. Long, D. McGraw, R. Miller, P. Lee, J. Perlin, D. Rucker, L. Sandy, L. Savage, L. Stump, P. Tang, E. Topol, R. Tuckson, and K. Valdes. 2022. The promise of digital health: Then, now, and the future. NAM Perspectives. Discussion Paper, National Academy of Medicine, Washington, DC. https://doi.org/10.31478/202206e.
Adler-Milstein, J. S. W. Rosenthal, R. Thombley, S. Rogers, B. Rosner, J. Yeh, and J. D. Harrison. 2025. From 4Ms to 5 domains: Ensuring new CMS Age-Friendly hospital measure improves care for older adults. Health Affairs Scholar 3(10). https://doi.org/10.1093/haschl/qxaf184.
AHRQ (Agency for Healthcare Research and Quality). 2024a.
AHRQ Strategic Plan for Health System Transformation to Optimize Health, Functional Status, and WellBeing Among Older Adults. Available at: https://www.ahrq.gov/ priority-populations/publications/aging-well.html (accessed December 19, 2025).
AHRQ. 2024b. Learning Health System Embedded Scientist Training and Research (LHS EStaR) Centers. Available at: https://www.ahrq.gov/ pcor/ahrq-pcor-trust-fund-training-projects/ pcor-lhs.html (accessed December 19, 2025).
AHRQ. n.d. PersonCentered Care Planning for People with Multiple Chronic Conditions (PCCP4P). Available at: https://www.ahrq. gov/sites/default/files/wysiwyg/mcc/pccp4p/ baseline-scan-report.pdf (accessed December 19, 2025).
Alberti, P., J. K. Bretsch, D. Oto-Kent, and K. M. King. 2025. To demonstrate trustworthiness, public health must listen, reflect, act, and revisit. American Journal of Public Health 116(1):86-89. https://doi.org/10.2105/AJPH.2025.308329.
American Geriatrics Society Expert Panel on Person-Centered Care. 2016. Person-centered care: A definition and essential elements. Journal of the American Geriatrics Society 64(1):15-18. https://doi.org/10.1111/jgs.13866.
American Hospital Association. 2017. Federal Agencies with Regulatory or Oversight Authority Impacting Hospitals. Available at: https://www. aha.org/system/files/2018-01/info-regulatory-burden-federal-agencies.pdf (accessed May 23, 2025).
Ashe, J. J., M. C. Baker, C. S. Alvarado, and P. M. Alberti. 2023. Screening for health-related social needs and collaboration with external partners among us hospitals. JAMA Network Open 6(8). https://doi.org/10.1001/ jamanetworkopen.2023.30228.
ASTP (Assistant Secretary for Technology Policy). 2023. Individuals’ access and use of patient portals and smartphone health apps, 2022. Available at: https://www.healthit.gov/data/data-briefs/individuals-access-and-use-patient-portals-and-smartphone-health-apps-2022 (accessed May 23, 2025).
Barry, M. J., and S. Edgman-Levitan. 2012. Shared decision making—The pinnacle of patient-centered care. The New England Journal of Medicine 366(9):780-781. https://doi. org/10.1056/NEJMp1109283.
Bellard, K. 2022. Health care execs behaving badly. Available at: https://thehealthcareblog.com/ blog/2022/09/29/health-care-execs-behaving-badly (accessed June 4, 2025).
Berkowitz, B. 2016. The patient experience and patient satisfaction: Measurement of a complex dynamic. The Online Journal of Nursing. https:// doi.org/10.3912/OJIN.Vol21No01Man01.
Bhatt, J., A. Davis, N. Batara, and B. Rush. 2022. US health care can’t afford health inequities. Available at: https://www.nationalforum.org/wp-content/uploads/2022/10/06.22.22-Jay-Bhatt-Article.pdf (accessed June 4, 2025).
Bierman, A. S., and K. B. Mistry. 2023. Commentary: Achieving health equity—The role of learning health systems. Healthcare Policy 19(2):21-27. https://doi.org/10.12927/hcpol.2023.27236.
Birkhäuer, J., J. Gaab, J. Kossowsky, S. Hasler, P. Krummenacher, C. Werner, and H. Gerger. 2017. Trust in the health care professional and health outcome: A meta-analysis. PLoS ONE 12(2):e0170988. https://doi.org/10.1371/ journal.pone.0170988.
Bloomberg Philanthropies. n.d. Building public health coalitions; partnership for healthy cities. Available at: https://www.bloomberg. org/public-health/building-public-health-coalitions/partnership-for-healthy-cities (accessed May 23, 2025).
Boroughs, B. 2024. How partnerships between organizations can transform a community for the better. Newsweek, March 13. Available at: https://www.newsweek.com/how-partnerships-between-organizations-can-transform-community-better-1878412 (accessed June 2, 2025).
Bradley, E. H., M. Canavan, E. Rogan, K. Talbert-Slagle, C. Ndumele, L. Taylor, and L. A. Curry. 2016. Spending on social services, public health, and health care, 2000–09. Health Affairs 35(5). https://doi.org/10.1377/hlthaff.2015.0814.
Bravemen, P. A., E. Arkin, D. Proctor, T. Kauh, and N. Holm. 2022. Systemic and structural racism: Definitions, examples, health damages, and approaches to dismantling. Health Affairs 41(2):171-178. https://doi.org/10.1377/ hlthaff.2021.01394.
Brown, A. M. 2017. Emergent strategy: Shaping change, changing worlds. Chico, CA: AK Press.
Brush, R. 2025. Change from within: A 10-year journey to improve health in five Wellville communities. Paper presented at Connecticut Children’s AY25 Pediatric Grand Rounds Honorary Dworkin Lecture, January 14, 2025, Hartford, CT. Available at: https://wellville.net/wp-content/uploads/2025/02/Change-from-Within_Presentation-on-January-14-2025.pdf (accessed February 25, 2026).
Brush, R. 2024. Learning from Communities on the Way to Wellville. Available at: https://wellville. net/to-shift-our-nations-health-we-need-to-shift-our-thinking-together (accessed June 2, 2025).
Burky, A. 2023. Healthcare ranked lowest for employee satisfaction, Qualtrics survey finds. Available at: https://www.fiercehealthcare. com/health-tech/qualtrics-survey-finds-only-half-healthcare-employees-think-they-are-paid-fairly (accessed June 3, 2025).
Cain, A., E. Ward, J. Murdoch, and N. Chakraborti. 2022. A snapshot of broadband access in rural communities. Available at: https://acf.gov/sites/default/files/documents/opre/broadband_special_topic_brief_jan2023.pdf (accessed June 4, 2025).
Casalino, L. P., S. Kariv, D. Markovits, R. Fisman, and
J. Li. 2024. Physician altruism and spending, hospital admissions, and emergency department visits. JAMA Health Forum 5(10). https://doi. org/10.1001/jamahealthforum.2024.3383.
CDC (Centers for Disease Control and Prevention). 2024. Principles of community engagement. 3rd ed. Washington, DC: CDC and Agency for Toxic Substances and Disease Registry. Available at: https://cohnlabs.org/principles-of-community-engagement (accessed May 27, 2025).
CDC. 2011. Principles of community engagement. 2nd ed. Washington, DC: National Institutes of Health. Available at: https://stacks.cdc. gov/view/cdc/11699 (accessed May 23, 2025).
Center for Health Incentives and Behavioral Economics. 2017. Healthcare finance: A healthier population will lead to lower healthcare costs, healthcare pros tell senate panel. Available at: https://chibe.upenn.edu/news/healthcare-finance-a-healthier-population-will-lead-to-lower-healthcare-costs-healthcare-pros-tell-senate-panel (accessed June 2, 2025).
Center on Social Disparities in Health, Build Healthy Places Network, and Robert Wood Johnson Foundation. 2015. How do neighborhood conditions shape health?: An excerpt from Making the Case for Linking Community Development and Health. Build Healthy Places Network. Available at: https://www.buildhealthyplaces.org/content/uploads/2015/09/How-Do-Neighborhood-Conditions-Shape-Health.pdf (accessed February 25, 2026).
Chan, R. J., V. E. Milch, F. Crawford-Williams, O.A. Agbejule, R. Joseph, J. Johal, N. Dick, M. P. Wallen, J. Ratcliffe, A. Agarwal, L. Nekhlyudov, M. Tieu, M. Al-Momani, S. Turnbull, R. Sathiaraj,
D. Keefe, and N. H. Hart. 2023. Patient navigation across the cancer care continuum: An overview of systematic reviews and emerging literature. CA: A Cancer Journal for Clinicians 73(6):565-589. https://doi.org/10.3322/caac.21788.
ChangeLab Solutions. 2019. A blueprint for changemakers: Achieving health equity through law and policy. Oakland, CA: ChangeLab Solutions.
Charlton, J. I. 1998. Nothing about us without us: Disability oppression and empowerment. Oakland, CA: University of California Press.
Chen, J., and Y. Wang. 2021. Social media use for health purposes: Systematic review. Journal of Medical Internet Research 23(5). https:// doi.org/10.2196/17917.
ChenMed. 2024. The role of trust in patient-provider collaboration. Available at: https:// www.chenmed.com/blog/role-trust-patient-provider-collaboration (accessed June 3, 2025).
Chinekezi, O., L. Andress, E. P. Agonafer, S. Massick, S. Piepenbrink, K. M. Sutton, P. M. Alberti,
D. de la Torre, S. Guillot-Wright, and M. Lee. 2023. From the national to the local: Issues of trust and a model for community-academic engagement. Frontiers in Public Health 11. https://doi.org/10.3389/fpubh.2023.1068425.
Chipidza, F. E., R. S. Wallwork, and T. A. Stern. 2015. Impact of the doctor–patient relationship. Primary Care Companion for CNS Disorders 17(5). https://doi.org/10.4088/PCC.15f01840.
City of Spartanburg. 2024. Hello Family shares transformative results, expands countywide. Available at: https://www.cityofspartanburg.org/CivicAlerts.aspx?AID=71 (accessed April 14, 2025).
CMS (Centers for Medicare and Medicaid Services). n.d. Accountable Health Communities Model. Available at: https://www.cms.gov/priorities/ innovation/innovation-models/ahcm (accessed May 23, 2025).
Collins, S., and T. Kaine. 2025. Senators Collins, Kaine introduce Geriatrics Workforce Improvement Act. Available at: https://www.collins.senate.gov/ newsroom/senators-collins-kaine-introduce-geriatrics-workforce-improvement-act (accessed December 19, 2025).
Columbia Gorge Health Council. n.d. Learn more about the Community Health Assessment (CHA) and Community Health Improvement Plan(CHIP). Available at: https://www.cghealthcouncil. org/cha-chip (accessed December 19, 2025).
Columbia Gorge Regional Community Health Assessment. 2013. Columbia Gorge Regional Community Health Assessment. Available at: https://static1.squarespace.com/static/5e7109f83cff1b7d10e22da6/t/5e726c1309d54f2db43c6b46/1584557083005/Columbia-Gorge-Community-Health-Assessment-December-2013.pdf (accessed December 19, 2025).
Connecticut Office of Health Strategy. 2019. Connecticut State Innovation Model (SIM) Health Enhancement Community Initiative proposed framework: Technical report. Hartford, CT: State of Connecticut Office of Health Strategy. County Health Rankings and Roadmaps. n.d. Explore Health Topics. Available at: https:// www.countyhealthrankings.org/what-impacts-health/model-of-health (accessed June 4, 2024).
Cramer, G. R., G. J. Young, S. Singh, J. McGuire, and D. Kim. 2021. Evidence that collaborative action between local health departments and nonprofit hospitals helps foster healthy behaviors in communities: A multilevel study. BMC Health Services Research 21(1). https:// doi.org/10.1186/s12913-020-05996-8.
Cronin, C. E., S. R. Singh, A. Burns, V. A. Yeager, N. Puro, T. Santos, A. Mathew, and B. Franz. 2024. Ohio presents opportunities for understanding hospital alignment with public health agencies on community health assessments. Health Affairs 43(6). https://doi.org/10.1377/hlthaff.2024.00017.
Delaware SHIP. 2025. Welcome Aboard! Available at: https://delawareship.org (accessed December
13, 2025).
Edelman, L. 2025. ‘Possibly the worst example of private equity greed’: In Prospect Medical bankruptcy, echoes of Steward. The Boston Globe, January 13. Available at: https://www. bostonglobe.com/2025/01/13/business/ prospect-medical-bankruptcy-private-equity/ (accessed June 4, 2025).
Engagement Scholarship Consortium. n.d. W. K. Kellogg Foundation Community Engagement Scholarship Awards. Available at: https:// engagementscholarship.org/grants-and-awards/the-w-k-kellogg-foundation-community-engagement-scholarship-award/ recipients/2023-w-k-kellogg-foundation-community-engagement-scholarship-awards (accessed June 2, 2025).
Everette, T. D., D. Sathasivam, and K. Siegel. 2023. Transformational Community Engagement to Advance Health Equity. Available at: https:// www.rwjf.org/en/insights/our-research/2023/01/ transformational-community-engagement-to-advance-health-equity.html (accessed June 2, 2025).
FDA (US Food and Drug Administration). 2022. Patient engagement in the design and conduct of medical device clinical studies. Available at: https://www.fda.gov/regulatory-information/ search-fda-guidance-documents/patient-engagement-design-and-conduct-medical-device-clinical-studies (accessed June 3, 2025).
Galanis, P., I. Moisoglou, A. Katsiroumpa, I. Vraka, O. Siskou, O. Konstantakopoulou, E. Meimeti, and D. Kaitelidou, E. Meimeti, and D. Kaitelidou. 2023. Increased job burnout and reduced job satisfaction for nurses compared to other healthcare workers after the COVID-19 pandemic. Nursing Reports 13(3):1090–1100. https://doi.org/10.3390/nursrep13030095.
Gebreyes, K., J. Bhatt, D. Rabinowitz, M. A. Williams, M. Keita, and W. Gerhardt. 2024. The US$2.8 Trillion Opportunity: How better health for all can drive US economic growth. Available at: https://www2.deloitte.com/us/en/insights/industry/health-care/health-equity-economic-impact.html (accessed June 3, 2025).
Glasberg, E. 2023. Narrative medicine teaches doctors how to listen to patients’ stories. Columbia News, June 5. Available at: https://news.columbia.edu/news/narrative-medicine-teaches-doctors-how-listen-patients-stories (accessed June 3, 2025).
Grob, R., G. Darien, and D. Meyer. 2019. Why physicians should trust in patients. JAMA 321(14):1347-1348. https://doi.org/10.1001/ jama.2019.1500.
Gunja, M. Z., E. D. Gumas, and R. D. Williams II. 2023. U.S. health care from a global perspective, 2022: Accelerating spending, worsening outcomes. Available at: https://www.commonwealthfund.org/publications/issue-briefs/2023/jan/us-health-care-global-perspective-2022 (acccessed June 3, 2025).
Health Affairs Forefront. 2023. Ahead of print: Evaluating CMS’s Accountable Health Communities Model’s effectiveness. Health Affairs Forefront. https://doi.org/10.1377/ forefront.20230515.871433.
Hekler, E., C. A. M. Anderson, and L. A. Cooper. 2022. Is it time to restructure the National Institutes of Health? American Journal of Public Health 112(7):965-968. https://doi.org/10.2105/AJPH.2022.306830.
HHS (US Department of Health and Human Services). 2022. Federal plan for equitable long-term recovery and resilience. Washington, DC: US Department of Health and Human Services. Available at: https://rippel.org/wp-content/ uploads/2025/02/Federal-Plan-for-Equitable-Long-Term-Recovery-and-Resilience-ELTRR-Full-Plan.pdf (accessed May 27, 2025).
HHS. 2021. Community health and economic prosperity: Engaging businessesasstewards and stakeholders. Washington, DC: US Department of Health and Human Services.
Homer, J., B. Milstein, G. B. Hirsch, and E. S. Fisher. 2016. Combined regional investments could substantially enhance health system performance and be financially affordable. Health Affairs 35(8). https://doi.org/10.1377/hlthaff.2015.1043.
Hoppe, T. A., A. Litovitz, K. A. Willis, R. A. Meseroll, M. J. Perkins, B. I. Hutchins, A. F. Davis, M. S. Lauer, H. A. Valantine, J. M. Anderson, and G. M. Santangelo. 2019. Topic choice contributes to the lower rate of NIH awards to African-American/black scientists. Science Advances 5(10). https://doi.org/10.1126/sciadv.aaw7238.
Hunter, J. D. 2024. Democracy and solidarity: On the cultural roots of America’s political crisis.
New Haven, CT: Yale University Press.
IRS (Internal Revenue Service). 2024. Community Health Needs Assessment for Charitable Hospital Organizations—Section 501(r)(3). Available at: https://www.irs.gov/charities-non-profits/community-health-needs-assessment-for-charitable-hospital-organizations-section-501r3 (accessed June 3, 2025).
Jabbarpour, Y., A. Jetty, H. Byun, A. Siddiqi, and J. Park. 2025. The health of US primary care: 2025 scorecard report—The cost of neglect. New York: Milbank Memorial Fund and The Physicians Foundation. https://doi.org/10.1599/ mmf.2025.0218.
Kaplan, R. M. 2019. More than medicine: The broken promise of American health. Cambridge, MA: Harvard University Press.
Kesler, J. T. 2000. Healthy communities and civil discourse: A leadership opportunity for public health professionals. Public Health Reports 115(2-3):238–242. https://stacks.cdc.gov/ view/cdc/64884.
Kimmerer, R. W. 2024. The serviceberry: Abundance and reciprocity in the natural world. Minneapolis, MN: Birchbark Books.
Klein, E., and D. Thompson. 2025. Abundance: On the experience of living in a world of information plenty. New York: Simon & Schuster.
Knowles, M., A. P. Crowley, A. Vasan, and S. Kangovi. 2023. Community health worker integration with and effectiveness in health care and public health in the United States. Annual Review of Public Health 44:363-381. https://doi. org/10.1146/annurev-publhealth-071521-031648.
Kresge Foundation. n.d. Community Investment for Health Equity. Available at: https://kresge. org/our-work/health/community-investment-in-health-equity (accessed June 3, 2025).
Kyle, M. A., and A. B. Frakt. 2021. Patient administrative burden in the US health care system. Health Services Research 56(5):755–765. https:doi. org/10.1111/1475-6773.13861.
Landry, E., and J. Sterman. 2017. The capability trap: Prevalence in human systems. Proceedings of the 35th International Conference of the System Dynamics Society 2:963-1010. Available at: https://proceedings.systemdynamics. org/2017/proceed/papers/P1325.pdf (accessed June 2, 2025).
Lawson, L. M. 2025. Thrive: How the science of the adolescent brain helps us imagine a better future for all children. New York: The New Press.
Lopes, L., A. Montero, M. Presiado, and L. Hamel. 2024. Americans’ challenges with health care costs. Available at: https://www.kff.org/health-costs/issue-brief/americans-challenges-with-health-care-costs (accessed June 2, 2025).
Madanat, H., A. Martinez, M. Molina, and G. Ayala. 2023. Impact of delivering a healthy lifestyle intervention: Promotora findings from Familias Sanas y Activas II. Journal of Health Science and Education 1(3):1–7. https://pmc.ncbi.nlm. nih.gov/articles/PMC10364119.
Martin, A., M. Hartman, B. Washington, and A. Catlin. 2024. National health expenditures in 2023: Faster growth as insurance coverage and utilization increased. Health Affairs 44(1):12-22. https://doi.org/10.1377/hlthaff.2024.01375.
Mathews, A. L., B. S. Coyle, and M. M. Deegan. 2015. Building community while complying with the Affordable Care Act in the Lehigh Valley of Pennsylvania. Progress in Community Health Partnerships: Research, Education, and Action 9(1):101-112. https://doi.org/10.1353/ cpr.2015.0000.
Maunder, R. G., N. D. Heeney, R. A. Greenberg, L. P. Jeffs, L. A. Wiesenfeld, J. Johnstone, and J. J. Hunter. 2023. The relationship between moral distress, burnout, and considering leaving a hospital job during the COVID-19 pandemic: A longitudinal survey. BMC Nursing 22:243. https://doi.org/10.1186/s12912-023-01407-5.
Maurer, M., R. Mangrum, T. Hilliard-Boone, A. Amolegbe, K. L. Carman, L. Forsythe, R. Mosbacher, J. K. Lesch, and K. Woodward. 2022. Understanding the influence and impact of stakeholder engagement in patient-centered outcomes research: A qualitative study. Journal of General Internal Medicine 37(Suppl 1):6–13. https://doi.org/10.1007/s11606-021-07104-w.
McGinnis, J. M., H. V. Fineberg, and V. J. Dzau. 2024. Shared commitments for health and health care: A trust framework from the learning health system. NAM Perspectives. Commentary, National Academy of Medicine, Washington, DC. https://doi.org/10.31478/202412c.
McGinnis, J. M., P. Williams-Russo, and J. R. Knickman. 2002. The case for more active policy attention to health promotion. Health Affairs (Millwood) 21(2):78-93. https://doi. org/10.1377/hlthaff.21.2.78.
Metcalf, L., and W. Casey. 2016. Game theory. In Cybersecurity and applied mathematics, edited by Donna Dickenson. Amsterdam: Elsevier. Pp. 63–73.
Milstein, B., J. Homer, B. Payne, and P. Reed. 2025. How can the United States make a great stride toward multiracial well-being? PLoS ONE 20(4): e0319320. https://doi.org/10.1371/journal.pone.0319320.
Milstein, B., J. Homer, and C. Soderquist. 2022. How can a community pursue equitable health and well-being after a severe shock? Ideas from an exploratory simulation model. Systems 10(5), 158. https://doi.org/10.3390/ systems10050158.
Milstein, B., B. Payne, C. Kelleher, J. Homer, T. Norris, M. Roulier, and S. Saha. 2023. Organizing around vital conditions moves the social determinants agenda into wider action. Health Affairs Forefront https://doi. org/10.1377/forefront.20230131.673841.
Minkler, M., and N. Wallerstein. 2008. Community-based participatory research for health: From process to outcomes. 2nd ed. San Francisco, CA: Jossey-Bass.
Mittmann, H., J. Heinrich, and J. Levi. 2022. Accountable communities for health: What we are learning from recent evaluations. NAM Perspectives. Discussion Paper, National Academy of Medicine, Washington, DC. https:// doi.org/10.31478/202210a.
NAM (National Academy of Medicine). n.d. Learning health system shared commitments. Available at: https://nam.edu/our-work/programs/ leadership-consortium/learning-health-system/ (accessed January 14, 2026).
National Association of County and City Health Officials. n.d. The Public Health System. Available at: https://www.naccho.org/uploads/ downloadable-resources/Programs/Public-Health-Infrastructure/Defining-Terms-The-Public-Health-System.pdf (accessed May 23, 2025)
NCATS (National Center for Advancing Translational Sciences). 2025. Community engagement across the CTSA program consortium. Available at: https://ncats.nih.gov/research/research-activities/ctsa/projects/community-engagement (accessed June 3, 2025).
NCHS (National Center for Health Statistics). 2020. Life expectancy estimates by U.S. Census tract, 2010-2015. https://www.cdc.gov/nchs/ data-visualization/life-expectancy (accessed May 23, 2025).
NIH CEAL (National Institutes of Health Community Engagement Alliance). n.d. NIH Community Engagement Alliance (CEAL). Available at: https://nihceal.org (accessed June 3, 2025).
OECD (Organisation for Economic Co-operation and Development). n.d. Health. OECD Better Life Index. https://www.oecdbetterlifeindex.org/topics/health (accessed June 3, 2025).
Organizing Committee for Assessing Meaningful Community Engagement in Health and Health Care Programs and Policies. 2022. Assessing Meaningful Community Engagement: A Conceptual Model to Advance Health Equity Through Transformed Systems for Health. NAM Perspectives. Commentary, National Academy of Medicine, Washington, DC. https://doi.org/10.31478/202202c.
Ostrom, E. 1990. Governing the commons: The evolution of institutions for collective action, New York: Cambridge University Press.
Partnership to Align Social Care. n.d. About Partnership to Align Social Care. Available at: https://www.partnership2asc.org/about (accessed April 14, 2025).
PCORI (Patient-Centered Outcomes Research Institute). 2023. Advisory Panel on Patient Engagement. Available at: https://www.pcori.org/ about/pcoris-advisory-panels/advisory-panel-patient-engagement (accessed June 3, 2025).
PCORI. 2015. Financial compensation of patients, caregivers, and patient/caregiver organizations engaged in PCORI-funded research as engaged research partners. Available at: https://www.pcori. org/sites/default/files/PCORI-Compensation-Framework-for-Engaged-Research-Partners.pdf (accessed April 14, 2025).
PCORI. n.d.-a. Eugene Washington PCORI Engagement Award Program. Available at: https://www.pcori.org/engagement-research/eugene-washington-pcori-engagement-award-program (accessed June 3, 2025).
PCORI. n.d.-b. Foundational expectations for partnerships in research. Available at: https://www.pcori.org/engagement-research/engagement-resources/foundational-expectations (accessed May 23, 2025).
PCORI. n.d.-c. Research fundamentals: Preparing you to successfully contribute to research. Available at: https://www.pcori.org/engagement-research/engagement-resources/research-fundamentals-preparing-you-successfully-contribute-research (accessed April 14, 2025). PCORI. n.d.-d. Building effective multi-stakeholder research teams. Available at: https://research-teams.pcori.org (accessed April 14, 2025).
PCORI. n.d.-e. Guide for engaging with research partners about data and analysis: Activities to support research partner involvement in data analysis and interpretation. Available at: https://www.pcori.org/sites/default/files/2021-09/PCORI-Guide-for-Engaging-with-Research-Partners-about-Data-and-Analysis.pdf (accessed April 14, 2025).
PCORI. n.d.-f. Engagement Tool and Resource Repository. Available at: https://www.pcori. org/engagement/engagement-resources/Engagement-Tool-Resource-Repository (accessed April 14, 2025).
Pferr, L. 2023. Community Care Hubs: What evidence-based program providers need to know. Available at: https://www.ncoa.org/article/community-care-hubs-what-evidence-based-program-providers-need-to-know (accessed June 3, 2025).
PHAB (Public Health Accreditation Board). 2016. Guide to National Public Health Department Reaccreditation: Process and Requirements. Available at: https://www.phaboard.org/wp-content/uploads/Guide-to-Reaccreditation-FINAL.pdf (accessed June 3, 2025).
Rakshit, S., and M. McGough, 2025. How does U.S. life expectancy compare to other countries? Available at: https://www.healthsystemtracker.org/chart-collection/u-s-life-expectancy-compare-countries (accessed June 2, 2025).
Research!America. 2022. U.S. investments in medical and health research and development: 2016–2020. Arlington, VA: Research!America.
Robert Wood Johnson Foundation. 2017. What is health equity? Available at: https://www.rwjf.org/en/insights/our-research/2017/05/what-is-health-equity-.html (accessed March 24, 2026).
RTI International. 2024. Accountable Health Communities (AHC) Model Evaluation: Third Evaluation Report. Baltimore, MD: Centers for Medicare & Medicaid Services (CMS).
Sandstrom, H., W. J. Congdon, M. Zhong, and F. Hernandez-Lepe. 2024. Spartanburg Hello Family Pay for Success Project Evaluation Design. Washington, DC: Urban Institute.
Scharmer, O., and P. Senge. 2016. Theory U: Leading from the Future as It Emerges. 2nd ed. Oakland, CA: Berrett-Koehler Publishers. https://www.oreilly.com/library/view/theory-u-2nd/9781626568006.
Sheche, J., S. Leekity, K. Lalio, C. Jim, K. Cartwright, and S. I. Mishra. 2024. Using community-based participatory research approaches to inform development of culturally appropriate cancer informational materials for the Pueblo of Zuni. Journal of Cancer Education 40:567-574. https://doi.org/10.1007/s13187-024-02544-4.
Shrank, W. H., T. L. Rogstad, and N. Parekh. 2019. Waste in the US health care system: Estimated costs and potential for savings. JAMA 322(15):1501-1509. https://doi.org/10.1001/jama.2019.13978.
Snyder, C. R., P. Z. Wang, and A. R. Truitt. 2018. Multiracial patient experiences with racial microaggressions in health care settings. Journal of Patient-Centered Research and Reviews 5(3):229–238. https://doi.org/10.17294/2330-0698.1626.
Sterling, R. L. 2011. Genetic research among the Havasupai: A cautionary tale. AMA Journal of Ethics 13(2):113-117. https://doi.org/10.1001/vi rtualmentor.2011.13.2.hlaw1-1102.
Stoneman, M., and M. McAninch. 2014. Providence Health & Services Oregon Region: 2013 Community Health Needs Assessments. Portland, OR: Providence Health & Services Available at: https://www.providence.org/-/media/Project/psjh/providence/socal/Files/ about/community-benefit/pdfs/2013chnaand chipprovidenceseasidehospital.pdf (accessed February 25, 2026).
Teisberg, E. O., S. Wallace, M. Ganz, C. T. Whitman, J. Hogan, R. Honigberg, A. Bosworth, D. Berwick,
D. Cosgrove, C. Fuller, C. M. Harris, J. Hill, M. Porter, F. Raines, F. Kennedy, N. Bartolucci, and M. McMurry. 2009. Health stewardship: The responsible path to a healthier nation. Washington, DC: Aspen Institute. https://search. issuelab.org/resource/health-stewardship-the-responsible-path-to-a-healthier-nation. html (accessed November 24, 2025).
Terrana, A., C. Viglione, K. Rhee, B. Rabin, J. Godino, G. A. Aarons, J. Chapman, B. Melendrez, M. Holguin, L. Osorio, P. Gidwani, C. J. Nunez, G. Firestein, and E. Hekler. 2024. The core functions and forms paradigm throughout EPIS: Designing and implementing an evidence-based practice with function fidelity. Frontiers in Health Services 3. https://doi.org/10.3389/ frhs.2023.1281690.
The Consilience Project. n.d. Development in Progress. Available at: https://consilienceproject.org/development-in-progress (accessed June 3, 2025).
The Rippel Foundation. n.d. Vital conditions for health and well-being. Available at: https://rippel.org/vital-conditions (accessed April 11, 2025).
US Department of the Treasury. 2024. U.S. Treasury announces $47 Million in awards from the SIPPRA program. Available at: https://home. treasury.gov/news/press-releases/jy2747 (accessed February 10, 2026).
US Government Accountability Office. 2021. Medicare: Information on the Transition to Alternative Payment Models by Providers in Rural, Health Professional Shortage, or Underserved Areas, GAO22104618. Washington, DC: US Government Accountability Office. Available at: https://www.gao.gov/products/ gao-22-104618 (accessed December 19, 2025).
Vogels, E. A. 2020. About one-in-five Americans use a smart watch or fitness tracker. Available at: https://www.pewresearch.org/short-reads/2020/01/09/about-one-in-five-americans-use-a-smart-watch-or-fitness-tracker (accessed June 3, 2020).
Wagner, E., I. Telesford, S. Rakshit, N. Kuranni, and C. Cox. 2024. How does the quality of the U.S. health system compare to other countries? Available at: https://www.healthsystemtracker. org/chart-collection/quality-u-s-healthcare-system-compare-countries (accessed June 3, 2025).
Washington State Health Care Authority. n.d. Accountable Communities of Health (ACHs). Available at: https://www.hca.wa.gov/about-hca/programs-and-initiatives/medicaid-transformation-project-mtp/accountable-communities-health-achs (accessed April 14, 2025).
Watson, B. N., L. Estenson, A. R. Eden, M. T. Gerstein, M. T. Carney, V. M. Dotson, T. Milnes, and A. S. Bierman. 2024. Person-centered care planning for people living with or at risk for multiple chronic conditions. JAMA Network Open 7(10). https://doi.org/10.1001/jamanetworkopen.2024.39851.
Wilkerson, I. 2020. Caste: The origins of our discontents. New York: Random House.
WHO. n.d. Constitution. Available at: https://www.who.int/about/governance/constitution (accessed May 23, 2025).
Yeung, A. W. K., A. Torkamani, A. J. Butte, B. S. Glicksberg, B. Schuller, B. Rodriguez, D.S.W. Ting, D. Bates, E. Schaden, H. Peng, H. Willschke, J. van der Laak, J. Car, K. Rahimi, L.A. Celi, M. Banach, M. Kletecka-Pulker, O. Kimberger, R. Eils, S.M.S. Islam, S.T. Wong, T.Y. Wong, W. Gao, S. Brunak, and A.G. Atanasov. 2023. The promise of digital healthcare technologies. Frontiers in Public Health 11. https://doi. org/10.3389/fpubh.2023.1196596.
Zhang, X., and R. Saltman. 2022. Impact of electronic health record interoperability on telehealth service outcomes. JMIR Medical Informatics 10(1):e31837. https://doi.org/10.2196/31837.
